The3-Level Acupuncture Protocol balances the Primary Channels (to regulate circulation of qi and blood), the Eight Extraordinary Channels (to regulate the musculoskeletal body), and the Divergent Channels (to regulate the internal zang-fu organs).If you haven’t read the previous blog posts in the 3-Level Acupuncture Balance series, you can get caught up here:THE 3-LEVEL ACUPUNCTURE BALANCE SERIES:
In this article, I will go into detail regarding the Divergent channels treatment. I am indebted to the attention and detail proposed by Miki Shima and Charles Chace in their book, The Channel Divergences, which I recommend for those seeking more and deeper information.
The Divergent channel balance examines differences of strength between the two channels in a yin-yang element pair, and prioritizes those pairs that are most out of balance for treatment. The AcuGraphoffers point recommendations that will put the yin-yang pairs back into balance. On the AcuGraph “Divergent” menu, it will be the second group of points offered, with preferred laterality.(It is preceded by the 8 Extra balance, which involves the first 3 or 4-point recommendations.)
By putting the yin-yang partners into balance, internal stress is reduced and zang-fu functionality is enhanced. Clinical application of Divergent channel treatment is rarely discussed in the modern TCM world, but Japanese acupuncturists revived and embellished the treatment during the 1970s and 1980s, to great effect.
Historical Development
The organization of divergent channels was first recorded in the Huang Di Nei Jing (“Yellow Emperor’s Internal Classic”, 2ndc. BCE), in the second part, the Ling Shu (“Spiritual Pivot”), Chapter 11, Jing Bie (“Channel Branches”). It describes in detail the branching and connecting of the paired channels by their anatomical locations. The pairs, in the order specified by in the Nei Jingare:
Foot Taiyang (BL) with Foot Shaoyin (KI) – water
Foot Shaoyang (GB) with Foot Jueyin (LV) – wood
Foot Yangming (ST) with Foot Taiyin (SP) – earth
Hand Taiyang (SI) with Hand Shaoyin (HT) – fire
Hand Shaoyang (TE) with Hand Jueyin (PC) – ministerial fire
Hand Yangming (LI) with Hand Taiyin (LU) – metal
Nei Jing(Ling Shu, Chapter 11) does not indicate at all what the function of these channels are, only the routing. It establishes the relationship of the yin and yang partner-channels of the six divisions. The term Jing Bie (经别 jīng bié) has stayed in use as the general term for the Divergent Channels, although “Branched Channels” would be a more accurate translation.
The take-home from the original Nei Jingdescription is the routing, placement, and sequence. These six pairs later were called Confluences, and the Nei Jing order became…
First Confluence (BL-KI)
Second Confluence (GB-LV)
Third Confluence (ST-SP)
Fourth Confluence (SI-HT)
Fifth Confluence (TE-PC)
Sixth Confluence (LI-LU)
Ling Shu Chapter 11 mapped out a general routing of the paired Confluences with places of intersection or crossing. Names of specific acupuncture points were not given, only general anatomical locations, such as “descends again to reach the Triple Warmer and scatters on the chest”, or, “ascends to communicate with the pharynx and links the root of the tongue”. Only later were specific acupoints names given.
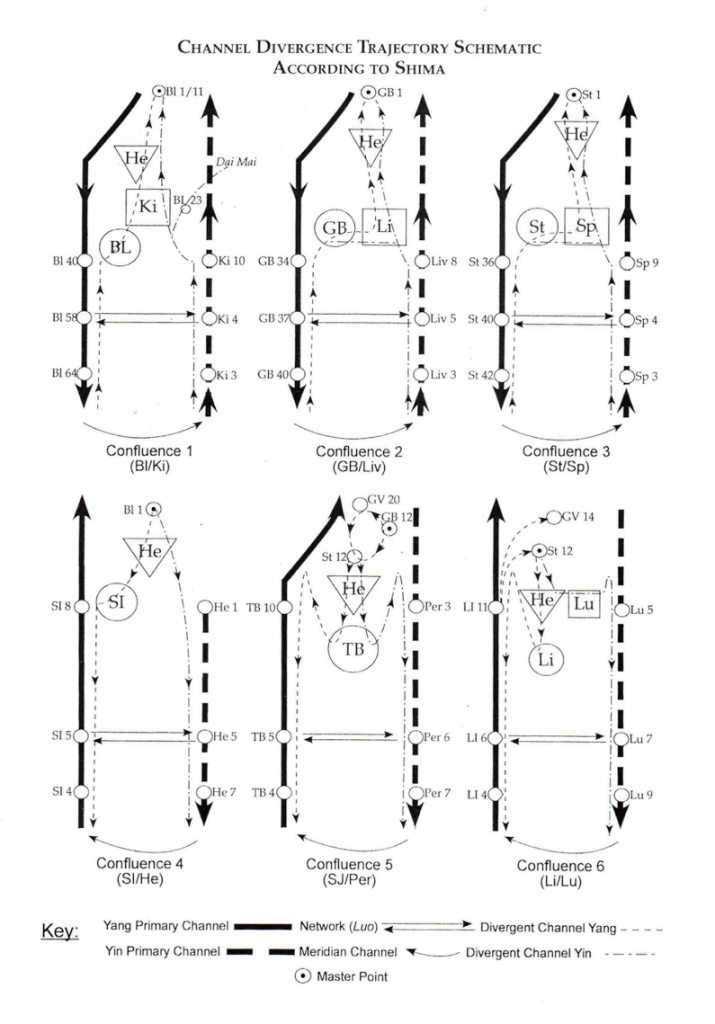
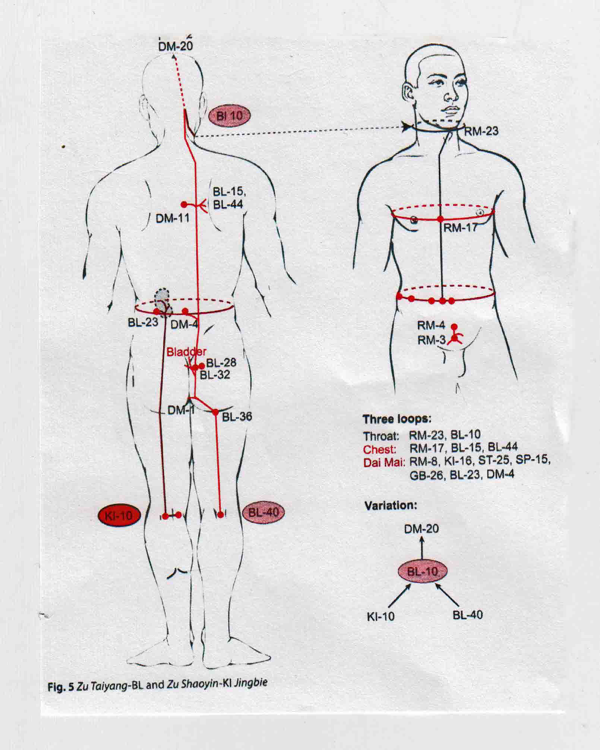
Miki Shima sums up the general routing in the following diagram (more specific locations with acupoints can be seen in Hamid Montakab’s diagrams at the end of this article).Basically the Divergent channel “diverges” or branches from the main channel to join with their yin-yang partner channel and organ.from The Channel Divergences, Shima and Chace, p. 32
The order of the Nei Jing Confluences, for me, led to several interesting observations. The first is that the pairs are anatomically in sequence, from lateral to medial. Starting with the foot, the most lateral pair of channels are BL and KI, then GB and LV, and finally, most medially is ST and SP. The same Confluence sequence, also lateral to medial, is found in the hand: the most lateral is SI and HT, then TE and PC, and finally, most medial, is LI and LU.
Secondly, the Confluences combine the yang and yin partnered-channels of the six divisions. The order for the yangchannels goes from lateral to medial: Taiyang, Shaoyang, Yangming.
The order (but not the Confluence order) for the yinchannels is the opposite, that is, medial to lateral: Taiyin, Jueyin and Shaoyin.
This sequence indicates the depth of the channels, with Taiyang (BL and SI) being the most superficial, and Shaoyin (HT and KI) being the deepest.
This sequence precedes, and is different from, the 2ndc. CE herbal classic Shang Han Lun, written by Zhang Zhong-Jing, who went Taiyang, Yangming, Shaoyang; Taiyin, Shaoyin, Jueyin.)
The Divergent channels regulate the distribution of qi, blood, yin, yang and fluids throughout the body. They actually allow interconnection between all the layers of energy and blood flow: the superficial(skin, musculo-tendino and luo-connecting channels), the middle layer(interstitial fascia, the lymphatics, the Primary channels), and the deepest layer: the internal zang-fu organs and the Eight Extraordinary channels (in the TCM orientation).
They are involved in pathogenic transmission of disease from the exterior to the organs, and offer a way to make sure pathogens don’t get to the internal zang-fu.
Conversely, disruptions in the internal zang-fu can emanate out through the layers to the exterior – think liver toxins affecting the skin. Any disruption in the body – wei, ying, and yuan layers – can be transferred in the Divergent channels.
The following observations are from noted scholars in the field of Divergent Channels.
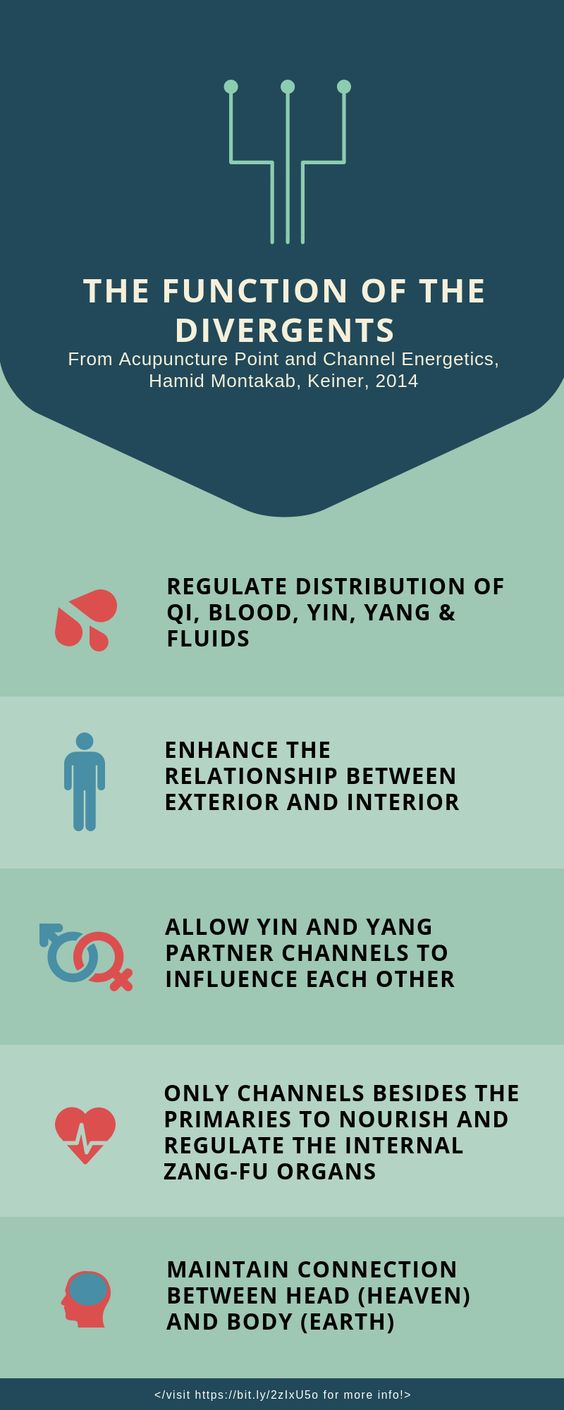
THE FUNCTION OF THE DIVERGENTS
From Acupuncture Point and Channel Energetics, Hamid Montakab, Keiner, 2014
Regulate distribution of qi, blood, yin, yang and fluids
Enhance the relationship between exterior and interior
Protect against pathogenic influences from diving deeper into body
Last protection against xie qi (pathogenic qi) penetrating to zang-fu
Deeper pathogens can get stuck at the divergent channel level, becoming latent or chronic pathogens
Allow yin and yang partner channels to influence each other
For example, LU 7 can influence the face, even though the channel does not surface at the face, by affecting the LI channel
Allows partner channel to take on excess or support deficiency
Only channels besides the Primaries to nourish and regulate the internal zang-fu organs
Maintain connection between head (heaven) and body (earth)
Helps connect head and neck with body and organs
Under stress, energy rises to head. Heaven and earth separate, and the root with the lower dantian is broken
Treatment brings excess above (neck and face) back down to he-sea points
FUNDAMENTALS OF THE DIVERGENT CHANNELS
according to David Twicken, The Divergent Channels, Singing Dragon, 2014
The Divergent Channels…
Branch out (separate) from the Primary Channels
Have no points of their own. They intersect with primary channels, and are influenced by those points
Strengthen the connections of the yin and yang partner channels. These connections determine the six Confluences. Most texts say that this is their most important function
Flow through the major joints of the body, especially those with large spaces
Pathogens are more easily stored in these spaces
Have an ascending or upwards direction, moving from the knees, hip and waist, chest, shoulders, and then the throat and face. This ascending action can move beneficial substances upwards (qi, blood, ying) but also can move pathogens upwards and outwards
Can interface interior and exterior, to bring vital substances or pathogens inwards, or force them outwards
Distribute qi to the neck, face, head and the sensory organs
Influence the three layers of the body: the superficial layer (wei qi); the middle layer (ying qi); and the deeper level (yuan qi)
Provide the internal connections of zang-fu organs to their sensory outlets (liver-eyes, lung-skin, heart-tongue, spleen-lips, kidney-ears)
Provide the internal connections of zang-fu organs to their emotional and psychological manifestations (liver: anger/depression; lung: grief; heart: excitement; spleen: pensiveness; kidney: fear; etc.)
CLINICAL APPLICATIONS ACCORDING TO TWICKEN
David Twicken, in The Divergent Channels (2014), carefully looks at the original Nei Jing Ling Shu, and finds six areas where the Divergent channels can be used clinically.
The Divergent Channels…
Treat conditions along their pathways, including areas where the Primary channels are not located
Treat their associated internal organs. The Divergents begin and end on the Primary channels, but they diverge to the associated partner yin or yang channel allowing them to treat the partner zang-fu
Treat conditions of their partner Primary channel, especially pathogenic factors. (Ling ShuChapter 10)
Treat conditions of their related luo-connecting channels, especially emotional conditions. (Ling Shu Chapter 10)
Treat conditions of the related musculo-tendino channels (Ling Shu Chapter 13)
Treats bone issues as they relate to muscles, tendons, eight extraordinary channels and yuan-jing. (Ling Shu Chapter 14)
Twicken’s clinical experience recommends treating many points along the Divergent channels, up to 8 points to cause a stronger reaction. His recommendations for treatment and diagnosis can be found in his book, The Divergent Channels.
FEATURES OF THE DIVERGENT CHANNELS
According to Wang Qi-cai, Secondary Channels and Collaterals, People’s Medical Publishing House, 2006
All twelve Divergents derive from the twelve Primary channels, but the originating and ending points and direction of qi flow are different
The yang divergent channels return to their own regular channels
The yin divergent channels join with their yang channel partners
The direction of the flow is always towards the center of the body
Twelve Divergents strengthen the relationship between the regular Primary channels and their pertaining organs
Distribute to places where the Primary channels do not go
Explain the interrelationship between Heart and Liver, Heart and Kidney, Heart and Spleen
Allow all six foot channels to communicate with the heart
Connect exterior and interior channels
Reinforce ability of luo-connecting channels to connect yang and yin partner channels
Connects all six yin channels to head, face, and sensory organs
Relationships with various tissues and organs
The 3 yang channels of the foot (BL, GB, ST) connect to the heart
ST (Foot Yangming) and GB (Foot Shaoyang) connect with the brain and the eyes
HT (Hand Shaoyin) goes to the inner canthus
PC (Hand Jueyin) connects to the ear
ST (Foot Yangming) connects to the mouth and lips
SP (Foot Taiyin) connects to the tongue
KI (Foot Shaoyin) connects to the root of the tongue
LU (Hand Taiyin), LI (Hand Yangming), ST (Foot Yangming), SP (Foot Taiyin), HT (Hand Shaoyin) and the GB (Foot Shaoyang) all connect to the throat
ST (Foot Yangming) and GB (Foot Shaoyang) connect to the esophagus
GB (Foot Shaoyang) enters the inguinal area
BL (Foot Tai yang) connects to the anus
CHARACTERISTICS AND OBSERVATIONS
According to Miki Shima and Charles Chace in The Channel Divergences, Blue Poppy, 2001
All Divergents travel proximally from the distal aspect on the extremities
This means that energy in the yang channels on the legs, and yin channels on the arm, are moving in a contrary direction to its associated Primary channel
Wei qi (defensive energy) basically runs distal to proximal, either in the Primary channel, or with the Divergent channel. The flow of wei qi inthe Divergent runs deeper than the Primary.
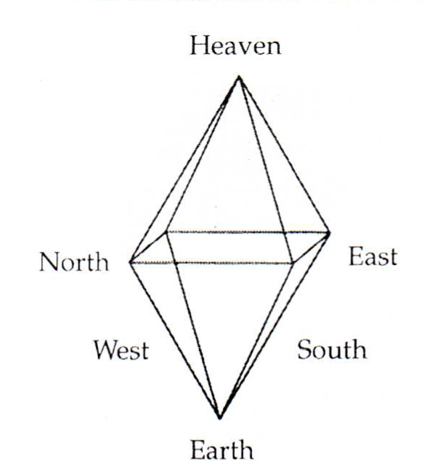
The Six Confluences, historically, correspond to the six directions (Heaven above, earth below, East, South, West, North). This also corresponds to Yoshio Manaka’s Octahedral model:
The qi that runs through the Divergents include wei qi, ying qi, yuan qi and jing qi
Some Japanese sources feel that it is the deepest of all the channel groups, which is why it can regulate the zang-fu organs
Western sources, including Joseph Helms, believe that it is wei qi that predominantly circulates through the Divergents
DIVERGENT CHANNEL DEVELOPMENT IN 20TH C. JAPAN
In a previous post, (Part 2 – Historical Development), I touched on the influences of the Topological Society on Divergent channel application in Japan. I’d like to talk about this in more depth.
The Topological Society consisted of acupuncturist-researchers gathered around Yoshio Manaka in the mid-20thcentury. Inspired by both Akabane and Manaka, they independently expanded the frontiers of channel theory and clinical applications of Eight Extraordinary channel theory. Several were also instrumental in reviving Divergent channel theory as a viable clinical application.
Collectively, they saw Divergent channels as a physically deeper meridian network, below the Primary channels. This network carried ying qi as well as yuan and jing qi. They proposed that more acute imbalances show on the Primary channels, while deeper and more chronic, with less severe symptoms, will show on the Divergent channels.
Divergent channel treatment was utilized to correct internal zang-fu imbalances, can correct yin-yang partner channel imbalances, and also to deal with pathogenic qithat has lodged deeper in the body. For all these reasons, including Divergent channel treatment is essential in our 3-Level Balance.
Participants in the Topological Society created detailed clinical applications for the Divergent channels. Basically, Divergent channel partners could be connected by combining specific extremity points with specific head/neck points. Using Manaka’s palpatory confirmation on the torso and extremities, they confirmed their clinical findings and treatments. For example, they found that unilateral treatments would correct imbalances on both sides.
TADASHI IRIE (1927-2002)
Irie studied with Yoshio Manaka, and became one of the leading voices concerning Divergent channel treatment. Irie established the head and neck master points for the Divergent Confluences, which have continued to stay in use. He proposed that at least two Confluences should be treated at a time.
Irie used Akabane incense diagnosis to look for the most unbalanced side of the Primary channels, and then transposed this to Divergent channel imbalance. In the 3-Level Balance protocol using the AcuGraph, these imbalances are clearly indicated in the Divergent menu(see my first post for further description of how to use AcuGraph to diagnose in the 3-Level Balance).The 3-Level Acupuncture Balance: Part 1- The Treatment >>
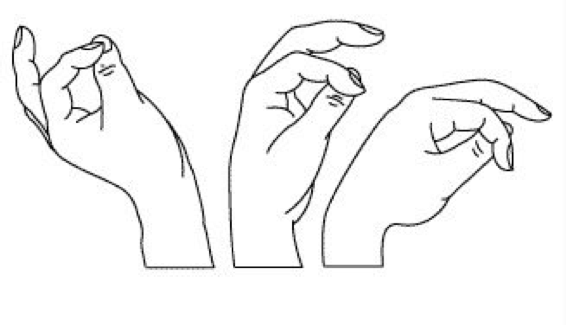
Irie had his own diagnostic feedback system to confirm his discoveries. These involved testing the friction/fluidity when rubbing his thumb and index finger together, similar to rubbing a rub plate.
In his method, one uses one hand to touch the acupuncture point or herbal substance. The other hand rubs the index finger over the top of the thumb. Slippery is a good response; sticky is a poor response.
One can also do this by rubbing the thumb on the side of the index finger. This is similar in principle to the Toftness technique in chiropractic.
Irie later developed a unique testing system for prioritizing the Confluences by placing six magnets across the forearm, diagnosing with either his sticky finger technique, or O-ring testing the patient. (See Shima and Chace, The Channel Divergences, p. 82-85.)
Irie’s work on the channel divergences was published in 1979, when he was 52 years old. Here he establish the head/neck points as the meeting points, that all subsequent Divergent practitioners have followed:
First Confluence, BL – KI BL 1 or BL 11
Second Confluence, GB – LV GB 1
Third Confluence, ST – SP ST 1
Fourth Confluence, SI – HT BL 1
Fifth Confluence, TE – PC GB 12
Sixth Confluence, LI – LU ST 12
(As I explained in my first blog post, I recommend substituting out a couple of these points because of needling concerns: BL 2 instead of BL 1, and ST 2 instead of ST 1. Actually, on ST 2, I do not use a needle because of the tendency to bleed; just placing the end of the Ion-pumping cord on the point, and securing with paper tape.)Irie recommended combining the head/neck point with an extremity point of the targeted channel. In this recommendation, Irie basically created our modern Divergent channel treatment. Later practitioners use ion-pumping cords (IPC) to facilitate and consolidate the treatment, although Irie and even Miki Shima did not.
Irie reaffirmed the Chinese classical indication that all Divergent channels had a proximal (superior) direction. When attaching ion-pumping cords between the leg he-sea points (at the knee), we place the black-end on the knee point, and the red-end on the head/neck points. This is in accord with the directional flow.
Irie also insisted that for the arm Divergent channels, the red pole is placed on the elbow he-sea point, and the black on the neck/head point, which seems to run counter to a proximal flow. Irie never explains why, but probably confirmed this via his finger-testing feedback system. One idea is that if the arms are held above the head, the flow would still be going in a proximal direction. This accords with the idea that yin channels flow upwards, from the ground up, and yang channels flow downwards, from heaven above towards the earth, if we hold our arms above our heads.Click here to buy ion pumping cords >>
In his 1979 publication, Irie’s diagnosis of which Divergent Confluence to choose was based on symptoms and palpation. If symptoms were diarrhea and abdominal pain, he would assume that this would be the 3rdConfluence (ST-SP). He would then palpate for pressure pain the torso Mu point (ST 25 or LV 13), as well as appropriate diagnostic points on their related channels (eg, SP 3, SP 4 or SP 9, and ST 36, ST 40 and ST 42).
In this way Irie would ascertain which of the paired channel was predominant, eg SP or ST. He would then treat the appropriate head/neck point with the appropriate polarity, and the sore point on the distal extremity. By treating the correct head/neck point, he would automatically direct a balance between the yinand yangpaired channels, eg, SP and ST.
Keep in mind that Irie was not committed to using the he-sea points that Shima uses in his SAT protocol, but would choose the sensitive pain/pressure point on the channel as the distal point to treat. In this regard our AcuGraph practitioners can, if they wish, also forgo the recommended he-seapoint and use other points of the channel that show up on palpation of muscle-testing.
As a footnote, Irie created the Kidney Return protocol that Miki Shima used later. This treats a deep Kidney deficiency, and is seen on many patients with adrenal weakness.
Tadashi Irie’s work on Divergents was the most sophisticated and comprehensive of the Topological Society’s contributors. His work profoundly influenced Miki Shima in the development of SAT therapy, and has filtered down to our own work in the 3-Level Balance.
KODO SEKI
Seki, originally a thoracic surgeon, had a large influence on the Topological Society’s development of Divergent channel therapy. Seki and Irie, in particular, influenced each other, and confirmed each other’s findings.
Seki’s selection of Divergent Confluences needing to be treated was based on pulse evaluation combined with pain-pressure reactivity on torso points and corresponding points on the arms and legs known as the Hirata Zones (see The Channel Divergences, p. 101). These were, in turn, directed by the patient’s complaints.
For treatment, Seki would combine Irie’s head/neck points with the corresponding yuan-source point on the related Divergent channel. Seki believed that the yuan-source point would access the original yuan qi, which would then influence the Divergent channel.
The author of Modern Electro-Acupuncture Therapeutics(1982), Seki would treat with rather strong electro-stim (7 Hz, 3 v, 5-10 minutes). After choosing the Confluence based on symptoms and palpatory diagnosis, he would choose electrical polarity based on symptoms.
For deficiency conditions, he would apply the negative pole to the yuan-source points of both yin and yang channels, and the positive pole to related Back-shu points.
For example, in lower back pain, he would apply the negative pole to KI 3 and BL 64, with the positive pole going to BL 28 (or BL 11) and BL 23. If the condition was an excess pattern, he would choose the same points, but use the opposite electrical polarity: positive for the yuan-source points, and negative for the Back-shu points.
Seki liked to treat either GV 20 (for the yang channels) or CV 22 (for the yin channels) on most patients. As he got older, he abandoned face and neck points altogether, and relied on GV 20 and CV 22 exclusively as Head master points. Seki later evolved to the point of using an ion-pumping cord to connect GV 20 to CV 22, using the patient’s O-ring test to determine polarity direction.
The technique of connecting GV 20 and CV 22 has survived in Miki Shima’s SAT protocol, as well our 3-Level protocol. Miki, who used silver and gold needles, would direct the qi from GV 20 towards CV 22. He felt most people had excess in the du mai, and deficiency in the ren mai. In our 3-Level protocol, I usually follow Miki’s lead, connecting GV 20 with an IPC (black) to CV 22 (red). This leads the qi forward in the microcosmic orbit, immediately regulating the yang and the yin. This promotes patient relaxation, and allows the brain to calm down.
SHIGEJI NAOMOTO (d. 1987)
Naomoto was an electrical engineer who built many of Manaka’s electrical acupuncture machines. His writings contributed to the Topological Society’s clinical application of Divergent channel therapy.
His primary diagnostic tool placed six different tuning forks on the palm of the patient, which he correlated with the Six Confluences. He then compared symptom and history to make his diagnosis. He also used facial diagnosis, abdominal palpation, O-ring testing, and range of motion before and after treatment. He may have been the first of the Japanese to promote Nogier’s ear acupuncture as an adjunct treatment.
Naomoto developed an electro-diagnostic device, which he used to compare measurements on the yin channels. He also revived the jin gei pulse diagnosis fromLing ShuChapter 48, where comparison is made between the carotid and radial arteries. Sensei Mutsuro Nakazono of the Kototama school of New Mexico also used this diagnostic method.
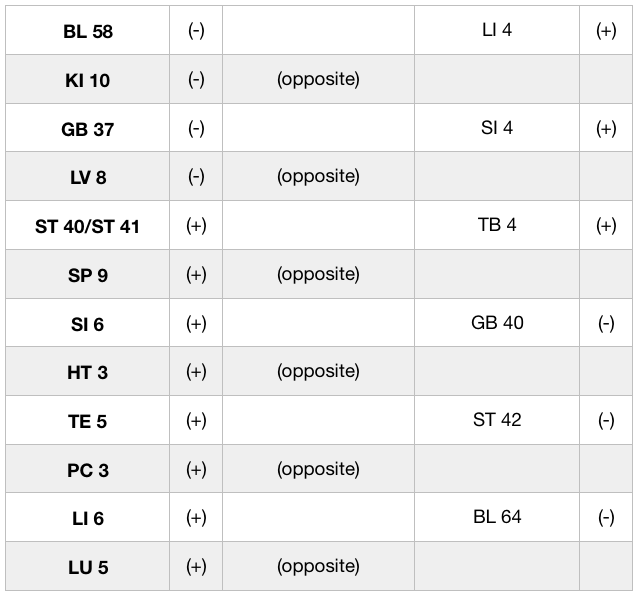
Naomoto promoted a Divergent channel protocol different from that of Kodo Seki. Whereas Seki, and others, utilized the head/neck points to connect the Divergent channel pair, Naomoto promoted a treatment that used the Midday-Midnight channel as the distal point.
He used his various diagnostic methods to determine the primary Confluence, and whether the yang or yin channel in a Confluence was the priority. He then chose the opposing channel on the Chinese clock as his combined point (instead of the head/neck point).
For example, if BL-KI (Confluence 1) is chosen, a needle is placed unilaterally on either the BL channel or the KI channel, depending on various diagnostic parameters. The opposite channel to the yin channel of the Confluence is chosen on the opposite limb, in this case LI. He used an ion-pumping cord in this way: for the first 3 Confluences, the channel divergence point is (-), and the opposite bio-clock point is (+). For the second 3 Confluences, the channel divergence point is (+) and the opposite bio-clock point is (-).
Naomoto’s Treatment Pairings:
These pairings can be used by AcuGraph users as an alternative to the Divergent menu recommendation.
MIKI SHIMA’S WORK ON DIVERGENT CHANNEL DIAGNOSIS AND TREATMENT
Miki Shima, working in California, took the work of Yoshio Manaka and the Topological Society, including Irie, Seki and Naomoto, and integrated their approach, with his own discoveries, into the SAT (Somato-Auricular Therapy).
Dr. Shima was first exposed to this work with the publication, in 1978, by Tadashi Irie’s articles in Ido-no-Nippon-Sha (Journal of Japanese Acupuncture and Moxibustion). Irie’s 1979 publication on Divergent channels defined the Master points on the head and neck. Shima brought Irie to the US to teach, and they created a close bond. When Shima expressed frustration at lack of a efficient diagnostic test for Divergent channel disorders, Irie suggested that Miki look into Akabane’s diagnostic method with incense and jing-well points.
Miki pursued this, in the process coming up with a way to diagnose not only Divergent channel imbalances, but Eight Extra Channel treatment as well. He also took note of Naomoto’s interest in auricular therapy, which would become a cornerstone of his the SAT approach.
Through his own clinical experience gathered in the 1980s, Dr. Shima determined that Irie’s Confluence head/neck points were preferable to Naomoto’s Midday-Midnight approach. He also settled on the he-sea points of the knee and elbow as the most clinically effective points. He felt that the qi of the channels dives deeper into the body at the he-sea points, and best influences the qi in the Divergent channels as it goes towards the zang-fu level.
Dr. Shima opposed Seki’s selection of yuan-source points as master points for the Divergents. The Nan Jing(66thchapter) stated that the yuan-source points are a way the yuan qi is distributed to the distal extremities. Shima felt these were too weak to distribute the deeper qi of the Divergents. Dr. Shima settled on the following point choices for Divergent treatment.
Divergent Confluences he-sea Points Head/Neck pointsFirst Confluence: BL 40 (-) or KI 10 (-) BL 1 (+)Second Confluence: GB 34 (-) or LV 8 (-) GB 1 (+)Third Confluence: ST 36 (-) or SP 9 (-) ST 1 (+)Fourth Confluence: SI 8 (+) or HT 3 (+) BL 1 (-)Fifth Confluence: TB 10 (+) or PC 3 (+) GB 12 (-)Sixth Confluence: LI 11 (+) or LU 5 (+) ST 12 (-)[In my 3-Level Acupuncture Balance, I propose variations on these point choices, basically using BL 2 instead of BL 1, and ST 2 instead of ST 1.]
SHIMA’S USE OF AKABANE TESTING
Miki Shima relied heavily on Akabane testing, although he would confirm, or otherwise change his findings, based on palpatory diagnosis on the channels or on the torso, as well as take into consideration the clinical and symptomatic manifestations.
But Akabane testing remained the foundation of his diagnosis, and our transposition of these findings into the AcuGraph form the basis of final point recommendations.
In traditional Akabane testing, an incense stick is swiped gently across the jing-well point for each meridian. The number of strokes is counted until the patient feels a burning heat sensation. These numbers are recorded for each channel, and each side of the body.
Shima, and Akabane, were concerned with the amount of yang energy in each channel, with pathology ensuing when the yang qi was excessive or deficient.
In the AcuGraph testing, we are measuring the amount of qi energy in the channel, not necessarily whether it’s yang energy or not.
Also, we are measuring at the yuan-source points, not the jing-well points. So said, once we have our findings on the AcuGraph, we are following Shima’s calculations to finalize the reading.
In a future post, I will explain how Dr. Shima utilized the Akabane readings to dictate point selection for both the Divergent channel treatment and the Eight Extraordinary channel treatment.
This is essentially the same procedure that Dr. Larsen used when creating the computerized readings.
MIKI SHIMA’S TREATMENT METHOD
After taking his Akabane readings and doing the calculations, Dr. Shima began his treatments first by clearing excesses and kori along the channels or abdomen with ses-sho-ku-shin manual techniques
He would then look at the Shu meridian pair to see the greatest divergence, and treat the weakest point on the weakest side, with either direct moxa or an intradermal needle.
For treatment of the 8 Extra and Divergents, he would follow Seki’s method. For the prioritized Confluences, he would needle the he-sea point of the yang channel on one side, and the he-sea point for the yin channel on the other side, using (-) for knee he-sea points, and (+) for elbow he-sea points.
The head/neck point would use the opposite polarity. The head/neck point would be unilateral, on the side of the yang channel.
For example, for the 2nd Confluence, he would needle GB 34 (-) on one side, LV 8 (-) on the other side, and GB 1 (+) on the same side as the yang channel, the side where GB 34 was placed.
AcuGraph users might choose this method, attaching two IPC, one from each he-sea point to the unilateral head/neck point. In my own practice, I find I am doing the he-sea point on the opposite limb, but not connecting with another IPC. Too many cords!
Shima did not use ion-pumping cords, preferring instead to use gold needles (+) and silver needles (-). He would often treat two or even three Confluences at the same time, and follow this with the Eight Extra channel treatment. He often used electro-stim, but not in weakened or hypersensitive patients.
Dr. Shima liked to use Irie’s Kidney Return Treatment with mild electro-stim. This was especially useful with very depleted kidney-deficient patients, the points being BL 40 (-), BL 23 (+), BL 11 (+).
On each side, two negative leads would emanate from BL 40, leading to BL 23 (+) and BL 11 (+). He chose to use 1 Hz, 5-10 milliamps, for 10 minutes.
In our 3-Level Protocol, this can also be done with IPC, or a combined electro-stim and IPC (BL 40 (-) > BL 23 (+) with electro stim; BL 40 (-) to BL 11 (+) with IPC).
Dr. Shima had many approaches in his tool chest, and was not rigid in his applications. A good number of case histories are included in his book, The Channel Divergences.
MY OWN THOUGHTS ON THE DIVERGENT CHANNEL TREATMENT
Our goal in assessing the Divergent Confluences is to see which yin-yang partners are most out of balance, and to repair that with a Divergent treatment.
The strategy is to choose the weakest of the two partners, and to hook that up to its head/neck meeting point. That will allow the partner, which is in excess, to flow into the most deficient of the paired channels.
For each recommended pair, there will be one he-sea point, coupled with a head or neck point. The he-sea point is on the affected channel (the weaker of the yin-yang Confluence pairs), but a single head or neck point, which is the meeting point for the two partners, is used by both partners in a Confluence.
If PC 3 and GB 12 are the indicated points on the AcuGraph Divergent menu, it means that PC is the weaker of the yin-yangpair, and PC 3 is the extremity he-sea point.
If TE was the weaker of the pair, then TE 10, the he-sea point, would be used, also with GB 12 as the head/neck point. But don’t consider GB 12 as the partner. It is the distal joining point, which is usually on an unrelated channel.
Finally, the AcuGraph menu dictates which side of the body should be used.
Two Confluences are always indicated. Sometimes it is recommend putting both treatments on the same side, which for purposes of balance, I usually don’t agree with.
I would like to see one Confluence treated on one side, and the other Confluence treated on the other side.What I would recommend is to look at those two pairs in a Confluence (by going to the “By Element” menu on the upper left side), and see if we can put one of the pairs on the other side.
If possible, support the treatment by choosing the he-sea point of the partner channel. For example, if PC 3 is treated on the left, treat TE 10 on the right. This will support the whole Divergent treatment.
By including the Divergent channel treatment with the Eight Extraordinary and Primary Channel treatments, using ion-pumping cords, we create a deep balance and invigorate the qi and blood in the body, using a minimum of needles.
DIAGRAMS OF THE CONFLUENCES
All drawings from Montakab, Acupuncture Point and Channel EnergeticsFirst Confluence, BL-KISecond Confluence, GB – LVThird Confluence, ST- SPFourth Confluence, SI – HTFifth Confluence TW – PESixth Confluence LI – LUBIBLIOGRAPHYAcupuncture Point and Channel Energetics, Hamid Montakab, Keiner, 2014
The Channel Divergences, Miki Shima and Charles Chace, Blue Poppy, 2001
The Divergent Channels, David Twicken, Singing Dragon, 2014
————————————————————————————————
Additional Resources
To learn more about ion pumping cords and the Divergent treatment, consider utilizing the resources below for more in-depth information, including a webinar series dedicated to the Divergent treatment and using ion pumping cords.
Part 2 of the Patients are Getting Better, Faster webinar includes an in-depth demonstration video of how to use ion pumping cords correctly. 1. Webinar: Patients are Getting Better, Faster (Be sure and register for both parts 1 and 2)2. Blog Post: Case Study: Ion Pumping Cords3. To purchase ion pumping cords, visit www.ioncords.com.
Other Posts in this Series
To read parts 1, 2, or 3 of the 3-Level Acupuncture Balance series, click the links below:
———————————————————————————————
Jake Paul Fratkin, OMD, L.Ac. trained in Korean and Japanese acupuncture since 1975, and Chinese herbal medicine since 1982. He is the author of Essential Chinese Formulas (2014), and Chinese Herbal Patent Medicines,The Clinical Desk Reference (2001). Jake practices in Boulder, Colorado, where he specializes in internal disorders, infections, and pediatrics.
Trained in Korean and Japanese acupuncture since 1975, and Chinese herbal medicine since 1982, and has studied and taught qi gong and Yang family Taijiquan since 1974. He is the author of Chinese Herbal Patent Medicines, The Clinical Desk Reference and the editor-organizer of Wu and Fischer’s Practical Therapeutics of Traditional Chinese Medicine. He is currently completing TCM Case Studies in Autoimmune Disease with Dr. Zeng Sheng-ping for People’s Medical Publishing House, Beijing. He is the recipient of Acupuncturist of the Year, 1999, by the AAAOM and Teacher of the Year, 2006, American Association of Teachers of Acupuncture and Oriental Medicine (AATAOM). Dr. Fratkin lives and practices in Boulder, Colorado.
View all posts by Dr. Jake P. Fratkin, DOM, L.Ac.
5 Replies to “The 3-Level Acupuncture Balance Part 4: More on the Divergent Channel Balance”
Jake, I always love learning from you. Your recognition and deep understanding of the divergent channel treatment, found within AcuGraph, has been a literal game changer with difficult patients. Thank you for your wisdom!
 The 3-Level Acupuncture Protocol balances the Primary Channels (to regulate circulation of qi and blood), the Eight Extraordinary Channels (to regulate the musculoskeletal body), and the Divergent Channels (to regulate the internal zang-fu organs).
If you haven’t read the previous blog posts in the 3-Level Acupuncture Balance series, you can get caught up here:
THE 3-LEVEL ACUPUNCTURE BALANCE SERIES:
The 3-Level Acupuncture Protocol balances the Primary Channels (to regulate circulation of qi and blood), the Eight Extraordinary Channels (to regulate the musculoskeletal body), and the Divergent Channels (to regulate the internal zang-fu organs).
If you haven’t read the previous blog posts in the 3-Level Acupuncture Balance series, you can get caught up here:
THE 3-LEVEL ACUPUNCTURE BALANCE SERIES:
 In this article, I will go into detail regarding the Divergent channels treatment. I am indebted to the attention and detail proposed by Miki Shima and Charles Chace in their book, The Channel Divergences, which I recommend for those seeking more and deeper information.
The Divergent channel balance examines differences of strength between the two channels in a yin-yang element pair, and prioritizes those pairs that are most out of balance for treatment. The AcuGraph offers point recommendations that will put the yin-yang pairs back into balance. On the AcuGraph “Divergent” menu, it will be the second group of points offered, with preferred laterality. (It is preceded by the 8 Extra balance, which involves the first 3 or 4-point recommendations.)
By putting the yin-yang partners into balance, internal stress is reduced and zang-fu functionality is enhanced. Clinical application of Divergent channel treatment is rarely discussed in the modern TCM world, but Japanese acupuncturists revived and embellished the treatment during the 1970s and 1980s, to great effect.
In this article, I will go into detail regarding the Divergent channels treatment. I am indebted to the attention and detail proposed by Miki Shima and Charles Chace in their book, The Channel Divergences, which I recommend for those seeking more and deeper information.
The Divergent channel balance examines differences of strength between the two channels in a yin-yang element pair, and prioritizes those pairs that are most out of balance for treatment. The AcuGraph offers point recommendations that will put the yin-yang pairs back into balance. On the AcuGraph “Divergent” menu, it will be the second group of points offered, with preferred laterality. (It is preceded by the 8 Extra balance, which involves the first 3 or 4-point recommendations.)
By putting the yin-yang partners into balance, internal stress is reduced and zang-fu functionality is enhanced. Clinical application of Divergent channel treatment is rarely discussed in the modern TCM world, but Japanese acupuncturists revived and embellished the treatment during the 1970s and 1980s, to great effect.
 From Acupuncture Point and Channel Energetics, Hamid Montakab, Keiner, 2014
From Acupuncture Point and Channel Energetics, Hamid Montakab, Keiner, 2014
 Branch out (separate) from the Primary Channels
Branch out (separate) from the Primary Channels All twelve Divergents derive from the twelve Primary channels, but the originating and ending points and direction of qi flow are different
All twelve Divergents derive from the twelve Primary channels, but the originating and ending points and direction of qi flow are different
 In a previous post, (Part 2 – Historical Development), I touched on the influences of the Topological Society on Divergent channel application in Japan. I’d like to talk about this in more depth.
The Topological Society consisted of acupuncturist-researchers gathered around Yoshio Manaka in the mid-20thcentury. Inspired by both Akabane and Manaka, they independently expanded the frontiers of channel theory and clinical applications of Eight Extraordinary channel theory. Several were also instrumental in reviving Divergent channel theory as a viable clinical application.
Collectively, they saw Divergent channels as a physically deeper meridian network, below the Primary channels. This network carried ying qi as well as yuan and jing qi. They proposed that more acute imbalances show on the Primary channels, while deeper and more chronic, with less severe symptoms, will show on the Divergent channels.
Divergent channel treatment was utilized to correct internal zang-fu imbalances, can correct yin-yang partner channel imbalances, and also to deal with pathogenic qithat has lodged deeper in the body. For all these reasons, including Divergent channel treatment is essential in our 3-Level Balance.
Participants in the Topological Society created detailed clinical applications for the Divergent channels. Basically, Divergent channel partners could be connected by combining specific extremity points with specific head/neck points. Using Manaka’s palpatory confirmation on the torso and extremities, they confirmed their clinical findings and treatments. For example, they found that unilateral treatments would correct imbalances on both sides.
In a previous post, (Part 2 – Historical Development), I touched on the influences of the Topological Society on Divergent channel application in Japan. I’d like to talk about this in more depth.
The Topological Society consisted of acupuncturist-researchers gathered around Yoshio Manaka in the mid-20thcentury. Inspired by both Akabane and Manaka, they independently expanded the frontiers of channel theory and clinical applications of Eight Extraordinary channel theory. Several were also instrumental in reviving Divergent channel theory as a viable clinical application.
Collectively, they saw Divergent channels as a physically deeper meridian network, below the Primary channels. This network carried ying qi as well as yuan and jing qi. They proposed that more acute imbalances show on the Primary channels, while deeper and more chronic, with less severe symptoms, will show on the Divergent channels.
Divergent channel treatment was utilized to correct internal zang-fu imbalances, can correct yin-yang partner channel imbalances, and also to deal with pathogenic qithat has lodged deeper in the body. For all these reasons, including Divergent channel treatment is essential in our 3-Level Balance.
Participants in the Topological Society created detailed clinical applications for the Divergent channels. Basically, Divergent channel partners could be connected by combining specific extremity points with specific head/neck points. Using Manaka’s palpatory confirmation on the torso and extremities, they confirmed their clinical findings and treatments. For example, they found that unilateral treatments would correct imbalances on both sides.
 Irie studied with Yoshio Manaka, and became one of the leading voices concerning Divergent channel treatment. Irie established the head and neck master points for the Divergent Confluences, which have continued to stay in use. He proposed that at least two Confluences should be treated at a time.
Irie used Akabane incense diagnosis to look for the most unbalanced side of the Primary channels, and then transposed this to Divergent channel imbalance. In the 3-Level Balance protocol using the AcuGraph, these imbalances are clearly indicated in the Divergent menu (see my first post for further description of how to use AcuGraph to diagnose in the 3-Level Balance).
The 3-Level Acupuncture Balance: Part 1- The Treatment >>
Irie had his own diagnostic feedback system to confirm his discoveries. These involved testing the friction/fluidity when rubbing his thumb and index finger together, similar to rubbing a rub plate.
In his method, one uses one hand to touch the acupuncture point or herbal substance. The other hand rubs the index finger over the top of the thumb. Slippery is a good response; sticky is a poor response.
One can also do this by rubbing the thumb on the side of the index finger. This is similar in principle to the Toftness technique in chiropractic.
Irie studied with Yoshio Manaka, and became one of the leading voices concerning Divergent channel treatment. Irie established the head and neck master points for the Divergent Confluences, which have continued to stay in use. He proposed that at least two Confluences should be treated at a time.
Irie used Akabane incense diagnosis to look for the most unbalanced side of the Primary channels, and then transposed this to Divergent channel imbalance. In the 3-Level Balance protocol using the AcuGraph, these imbalances are clearly indicated in the Divergent menu (see my first post for further description of how to use AcuGraph to diagnose in the 3-Level Balance).
The 3-Level Acupuncture Balance: Part 1- The Treatment >>
Irie had his own diagnostic feedback system to confirm his discoveries. These involved testing the friction/fluidity when rubbing his thumb and index finger together, similar to rubbing a rub plate.
In his method, one uses one hand to touch the acupuncture point or herbal substance. The other hand rubs the index finger over the top of the thumb. Slippery is a good response; sticky is a poor response.
One can also do this by rubbing the thumb on the side of the index finger. This is similar in principle to the Toftness technique in chiropractic.
 Irie later developed a unique testing system for prioritizing the Confluences by placing six magnets across the forearm, diagnosing with either his sticky finger technique, or O-ring testing the patient. (See Shima and Chace, The Channel Divergences, p. 82-85.)
Irie’s work on the channel divergences was published in 1979, when he was 52 years old. Here he establish the head/neck points as the meeting points, that all subsequent Divergent practitioners have followed:
Irie later developed a unique testing system for prioritizing the Confluences by placing six magnets across the forearm, diagnosing with either his sticky finger technique, or O-ring testing the patient. (See Shima and Chace, The Channel Divergences, p. 82-85.)
Irie’s work on the channel divergences was published in 1979, when he was 52 years old. Here he establish the head/neck points as the meeting points, that all subsequent Divergent practitioners have followed:
 Irie recommended combining the head/neck point with an extremity point of the targeted channel. In this recommendation, Irie basically created our modern Divergent channel treatment. Later practitioners use ion-pumping cords (IPC) to facilitate and consolidate the treatment, although Irie and even Miki Shima did not.
Irie reaffirmed the Chinese classical indication that all Divergent channels had a proximal (superior) direction. When attaching ion-pumping cords between the leg he-sea points (at the knee), we place the black-end on the knee point, and the red-end on the head/neck points. This is in accord with the directional flow.
Irie also insisted that for the arm Divergent channels, the red pole is placed on the elbow he-sea point, and the black on the neck/head point, which seems to run counter to a proximal flow. Irie never explains why, but probably confirmed this via his finger-testing feedback system. One idea is that if the arms are held above the head, the flow would still be going in a proximal direction. This accords with the idea that yin channels flow upwards, from the ground up, and yang channels flow downwards, from heaven above towards the earth, if we hold our arms above our heads.
Click here to buy ion pumping cords >>
In his 1979 publication, Irie’s diagnosis of which Divergent Confluence to choose was based on symptoms and palpation. If symptoms were diarrhea and abdominal pain, he would assume that this would be the 3rdConfluence (ST-SP). He would then palpate for pressure pain the torso Mu point (ST 25 or LV 13), as well as appropriate diagnostic points on their related channels (eg, SP 3, SP 4 or SP 9, and ST 36, ST 40 and ST 42).
In this way Irie would ascertain which of the paired channel was predominant, eg SP or ST. He would then treat the appropriate head/neck point with the appropriate polarity, and the sore point on the distal extremity. By treating the correct head/neck point, he would automatically direct a balance between the yinand yangpaired channels, eg, SP and ST.
Keep in mind that Irie was not committed to using the he-sea points that Shima uses in his SAT protocol, but would choose the sensitive pain/pressure point on the channel as the distal point to treat. In this regard our AcuGraph practitioners can, if they wish, also forgo the recommended he-seapoint and use other points of the channel that show up on palpation of muscle-testing.
As a footnote, Irie created the Kidney Return protocol that Miki Shima used later. This treats a deep Kidney deficiency, and is seen on many patients with adrenal weakness.
Tadashi Irie’s work on Divergents was the most sophisticated and comprehensive of the Topological Society’s contributors. His work profoundly influenced Miki Shima in the development of SAT therapy, and has filtered down to our own work in the 3-Level Balance.
Irie recommended combining the head/neck point with an extremity point of the targeted channel. In this recommendation, Irie basically created our modern Divergent channel treatment. Later practitioners use ion-pumping cords (IPC) to facilitate and consolidate the treatment, although Irie and even Miki Shima did not.
Irie reaffirmed the Chinese classical indication that all Divergent channels had a proximal (superior) direction. When attaching ion-pumping cords between the leg he-sea points (at the knee), we place the black-end on the knee point, and the red-end on the head/neck points. This is in accord with the directional flow.
Irie also insisted that for the arm Divergent channels, the red pole is placed on the elbow he-sea point, and the black on the neck/head point, which seems to run counter to a proximal flow. Irie never explains why, but probably confirmed this via his finger-testing feedback system. One idea is that if the arms are held above the head, the flow would still be going in a proximal direction. This accords with the idea that yin channels flow upwards, from the ground up, and yang channels flow downwards, from heaven above towards the earth, if we hold our arms above our heads.
Click here to buy ion pumping cords >>
In his 1979 publication, Irie’s diagnosis of which Divergent Confluence to choose was based on symptoms and palpation. If symptoms were diarrhea and abdominal pain, he would assume that this would be the 3rdConfluence (ST-SP). He would then palpate for pressure pain the torso Mu point (ST 25 or LV 13), as well as appropriate diagnostic points on their related channels (eg, SP 3, SP 4 or SP 9, and ST 36, ST 40 and ST 42).
In this way Irie would ascertain which of the paired channel was predominant, eg SP or ST. He would then treat the appropriate head/neck point with the appropriate polarity, and the sore point on the distal extremity. By treating the correct head/neck point, he would automatically direct a balance between the yinand yangpaired channels, eg, SP and ST.
Keep in mind that Irie was not committed to using the he-sea points that Shima uses in his SAT protocol, but would choose the sensitive pain/pressure point on the channel as the distal point to treat. In this regard our AcuGraph practitioners can, if they wish, also forgo the recommended he-seapoint and use other points of the channel that show up on palpation of muscle-testing.
As a footnote, Irie created the Kidney Return protocol that Miki Shima used later. This treats a deep Kidney deficiency, and is seen on many patients with adrenal weakness.
Tadashi Irie’s work on Divergents was the most sophisticated and comprehensive of the Topological Society’s contributors. His work profoundly influenced Miki Shima in the development of SAT therapy, and has filtered down to our own work in the 3-Level Balance.
 These pairings can be used by AcuGraph users as an alternative to the Divergent menu recommendation.
These pairings can be used by AcuGraph users as an alternative to the Divergent menu recommendation.
 Miki Shima, working in California, took the work of Yoshio Manaka and the Topological Society, including Irie, Seki and Naomoto, and integrated their approach, with his own discoveries, into the SAT (Somato-Auricular Therapy).
Dr. Shima was first exposed to this work with the publication, in 1978, by Tadashi Irie’s articles in Ido-no-Nippon-Sha (Journal of Japanese Acupuncture and Moxibustion). Irie’s 1979 publication on Divergent channels defined the Master points on the head and neck. Shima brought Irie to the US to teach, and they created a close bond. When Shima expressed frustration at lack of a efficient diagnostic test for Divergent channel disorders, Irie suggested that Miki look into Akabane’s diagnostic method with incense and jing-well points.
Miki pursued this, in the process coming up with a way to diagnose not only Divergent channel imbalances, but Eight Extra Channel treatment as well. He also took note of Naomoto’s interest in auricular therapy, which would become a cornerstone of his the SAT approach.
Through his own clinical experience gathered in the 1980s, Dr. Shima determined that Irie’s Confluence head/neck points were preferable to Naomoto’s Midday-Midnight approach. He also settled on the he-sea points of the knee and elbow as the most clinically effective points. He felt that the qi of the channels dives deeper into the body at the he-sea points, and best influences the qi in the Divergent channels as it goes towards the zang-fu level.
Dr. Shima opposed Seki’s selection of yuan-source points as master points for the Divergents. The Nan Jing (66thchapter) stated that the yuan-source points are a way the yuan qi is distributed to the distal extremities. Shima felt these were too weak to distribute the deeper qi of the Divergents. Dr. Shima settled on the following point choices for Divergent treatment.
Divergent Confluences he-sea Points Head/Neck points
First Confluence: BL 40 (-) or KI 10 (-) BL 1 (+)
Second Confluence: GB 34 (-) or LV 8 (-) GB 1 (+)
Third Confluence: ST 36 (-) or SP 9 (-) ST 1 (+)
Fourth Confluence: SI 8 (+) or HT 3 (+) BL 1 (-)
Fifth Confluence: TB 10 (+) or PC 3 (+) GB 12 (-)
Sixth Confluence: LI 11 (+) or LU 5 (+) ST 12 (-)
[In my 3-Level Acupuncture Balance, I propose variations on these point choices, basically using BL 2 instead of BL 1, and ST 2 instead of ST 1.]
Miki Shima, working in California, took the work of Yoshio Manaka and the Topological Society, including Irie, Seki and Naomoto, and integrated their approach, with his own discoveries, into the SAT (Somato-Auricular Therapy).
Dr. Shima was first exposed to this work with the publication, in 1978, by Tadashi Irie’s articles in Ido-no-Nippon-Sha (Journal of Japanese Acupuncture and Moxibustion). Irie’s 1979 publication on Divergent channels defined the Master points on the head and neck. Shima brought Irie to the US to teach, and they created a close bond. When Shima expressed frustration at lack of a efficient diagnostic test for Divergent channel disorders, Irie suggested that Miki look into Akabane’s diagnostic method with incense and jing-well points.
Miki pursued this, in the process coming up with a way to diagnose not only Divergent channel imbalances, but Eight Extra Channel treatment as well. He also took note of Naomoto’s interest in auricular therapy, which would become a cornerstone of his the SAT approach.
Through his own clinical experience gathered in the 1980s, Dr. Shima determined that Irie’s Confluence head/neck points were preferable to Naomoto’s Midday-Midnight approach. He also settled on the he-sea points of the knee and elbow as the most clinically effective points. He felt that the qi of the channels dives deeper into the body at the he-sea points, and best influences the qi in the Divergent channels as it goes towards the zang-fu level.
Dr. Shima opposed Seki’s selection of yuan-source points as master points for the Divergents. The Nan Jing (66thchapter) stated that the yuan-source points are a way the yuan qi is distributed to the distal extremities. Shima felt these were too weak to distribute the deeper qi of the Divergents. Dr. Shima settled on the following point choices for Divergent treatment.
Divergent Confluences he-sea Points Head/Neck points
First Confluence: BL 40 (-) or KI 10 (-) BL 1 (+)
Second Confluence: GB 34 (-) or LV 8 (-) GB 1 (+)
Third Confluence: ST 36 (-) or SP 9 (-) ST 1 (+)
Fourth Confluence: SI 8 (+) or HT 3 (+) BL 1 (-)
Fifth Confluence: TB 10 (+) or PC 3 (+) GB 12 (-)
Sixth Confluence: LI 11 (+) or LU 5 (+) ST 12 (-)
[In my 3-Level Acupuncture Balance, I propose variations on these point choices, basically using BL 2 instead of BL 1, and ST 2 instead of ST 1.]
 After taking his Akabane readings and doing the calculations, Dr. Shima began his treatments first by clearing excesses and kori along the channels or abdomen with ses-sho-ku-shin manual techniques
He would then look at the Shu meridian pair to see the greatest divergence, and treat the weakest point on the weakest side, with either direct moxa or an intradermal needle.
For treatment of the 8 Extra and Divergents, he would follow Seki’s method. For the prioritized Confluences, he would needle the he-sea point of the yang channel on one side, and the he-sea point for the yin channel on the other side, using (-) for knee he-sea points, and (+) for elbow he-sea points.
The head/neck point would use the opposite polarity. The head/neck point would be unilateral, on the side of the yang channel.
For example, for the 2nd Confluence, he would needle GB 34 (-) on one side, LV 8 (-) on the other side, and GB 1 (+) on the same side as the yang channel, the side where GB 34 was placed.
AcuGraph users might choose this method, attaching two IPC, one from each he-sea point to the unilateral head/neck point. In my own practice, I find I am doing the he-sea point on the opposite limb, but not connecting with another IPC. Too many cords!
Shima did not use ion-pumping cords, preferring instead to use gold needles (+) and silver needles (-). He would often treat two or even three Confluences at the same time, and follow this with the Eight Extra channel treatment. He often used electro-stim, but not in weakened or hypersensitive patients.
Dr. Shima liked to use Irie’s Kidney Return Treatment with mild electro-stim. This was especially useful with very depleted kidney-deficient patients, the points being BL 40 (-), BL 23 (+), BL 11 (+).
On each side, two negative leads would emanate from BL 40, leading to BL 23 (+) and BL 11 (+). He chose to use 1 Hz, 5-10 milliamps, for 10 minutes.
In our 3-Level Protocol, this can also be done with IPC, or a combined electro-stim and IPC (BL 40 (-) > BL 23 (+) with electro stim; BL 40 (-) to BL 11 (+) with IPC).
Dr. Shima had many approaches in his tool chest, and was not rigid in his applications. A good number of case histories are included in his book, The Channel Divergences.
After taking his Akabane readings and doing the calculations, Dr. Shima began his treatments first by clearing excesses and kori along the channels or abdomen with ses-sho-ku-shin manual techniques
He would then look at the Shu meridian pair to see the greatest divergence, and treat the weakest point on the weakest side, with either direct moxa or an intradermal needle.
For treatment of the 8 Extra and Divergents, he would follow Seki’s method. For the prioritized Confluences, he would needle the he-sea point of the yang channel on one side, and the he-sea point for the yin channel on the other side, using (-) for knee he-sea points, and (+) for elbow he-sea points.
The head/neck point would use the opposite polarity. The head/neck point would be unilateral, on the side of the yang channel.
For example, for the 2nd Confluence, he would needle GB 34 (-) on one side, LV 8 (-) on the other side, and GB 1 (+) on the same side as the yang channel, the side where GB 34 was placed.
AcuGraph users might choose this method, attaching two IPC, one from each he-sea point to the unilateral head/neck point. In my own practice, I find I am doing the he-sea point on the opposite limb, but not connecting with another IPC. Too many cords!
Shima did not use ion-pumping cords, preferring instead to use gold needles (+) and silver needles (-). He would often treat two or even three Confluences at the same time, and follow this with the Eight Extra channel treatment. He often used electro-stim, but not in weakened or hypersensitive patients.
Dr. Shima liked to use Irie’s Kidney Return Treatment with mild electro-stim. This was especially useful with very depleted kidney-deficient patients, the points being BL 40 (-), BL 23 (+), BL 11 (+).
On each side, two negative leads would emanate from BL 40, leading to BL 23 (+) and BL 11 (+). He chose to use 1 Hz, 5-10 milliamps, for 10 minutes.
In our 3-Level Protocol, this can also be done with IPC, or a combined electro-stim and IPC (BL 40 (-) > BL 23 (+) with electro stim; BL 40 (-) to BL 11 (+) with IPC).
Dr. Shima had many approaches in his tool chest, and was not rigid in his applications. A good number of case histories are included in his book, The Channel Divergences.
 What I would recommend is to look at those two pairs in a Confluence (by going to the “By Element” menu on the upper left side), and see if we can put one of the pairs on the other side.
If possible, support the treatment by choosing the he-sea point of the partner channel. For example, if PC 3 is treated on the left, treat TE 10 on the right. This will support the whole Divergent treatment.
By including the Divergent channel treatment with the Eight Extraordinary and Primary Channel treatments, using ion-pumping cords, we create a deep balance and invigorate the qi and blood in the body, using a minimum of needles.
What I would recommend is to look at those two pairs in a Confluence (by going to the “By Element” menu on the upper left side), and see if we can put one of the pairs on the other side.
If possible, support the treatment by choosing the he-sea point of the partner channel. For example, if PC 3 is treated on the left, treat TE 10 on the right. This will support the whole Divergent treatment.
By including the Divergent channel treatment with the Eight Extraordinary and Primary Channel treatments, using ion-pumping cords, we create a deep balance and invigorate the qi and blood in the body, using a minimum of needles.
 First Confluence, BL-KI
First Confluence, BL-KI
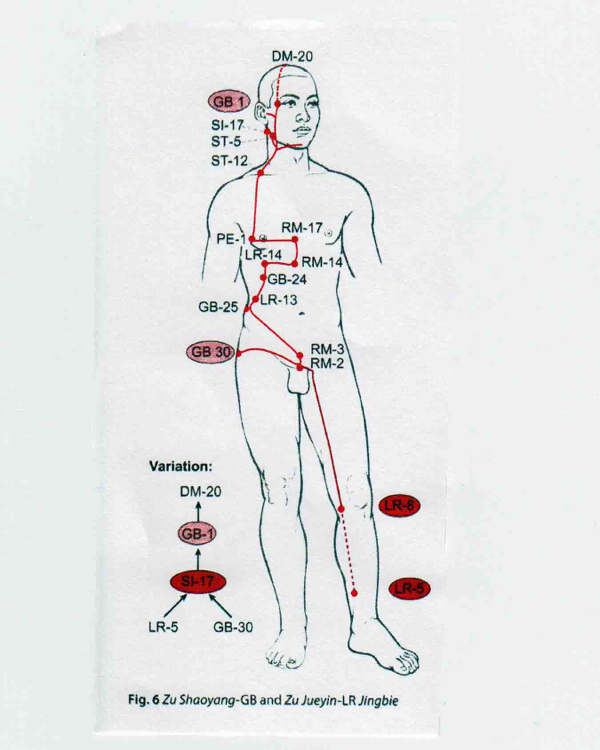 Second Confluence, GB – LV
Second Confluence, GB – LV
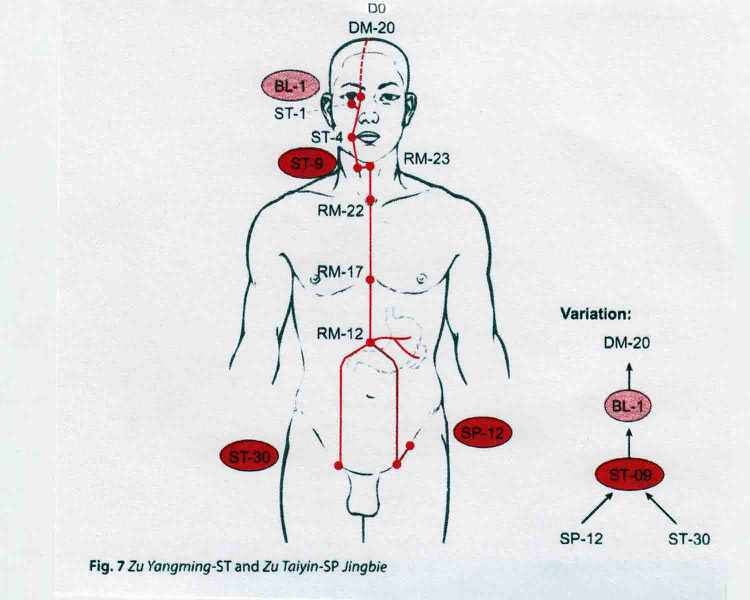 Third Confluence, ST- SP
Third Confluence, ST- SP
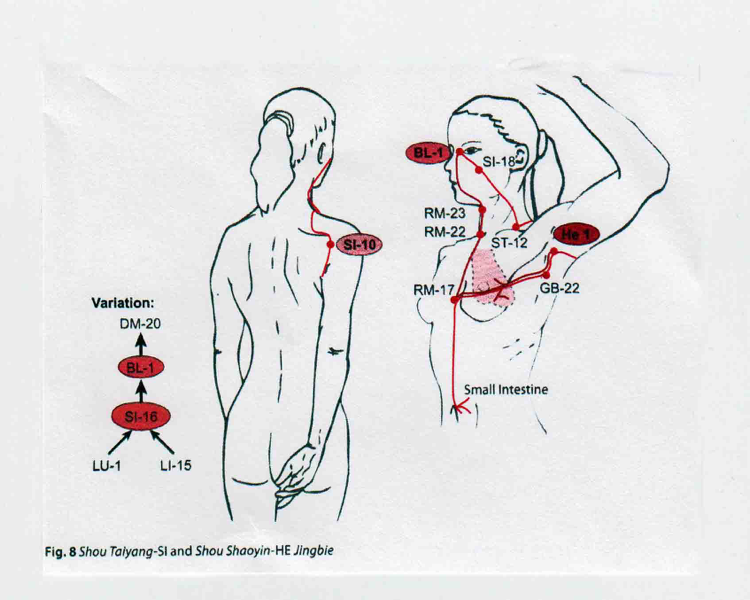 Fourth Confluence, SI – HT
Fourth Confluence, SI – HT
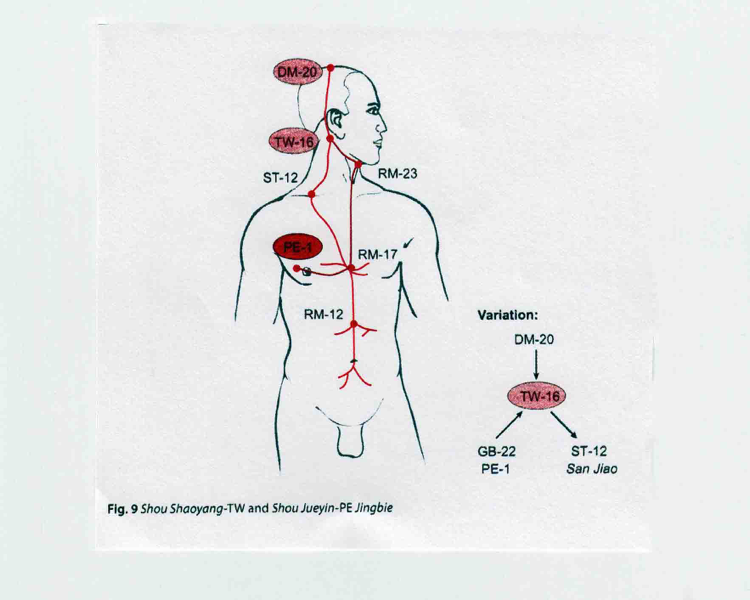 Fifth Confluence TW – PE
Fifth Confluence TW – PE
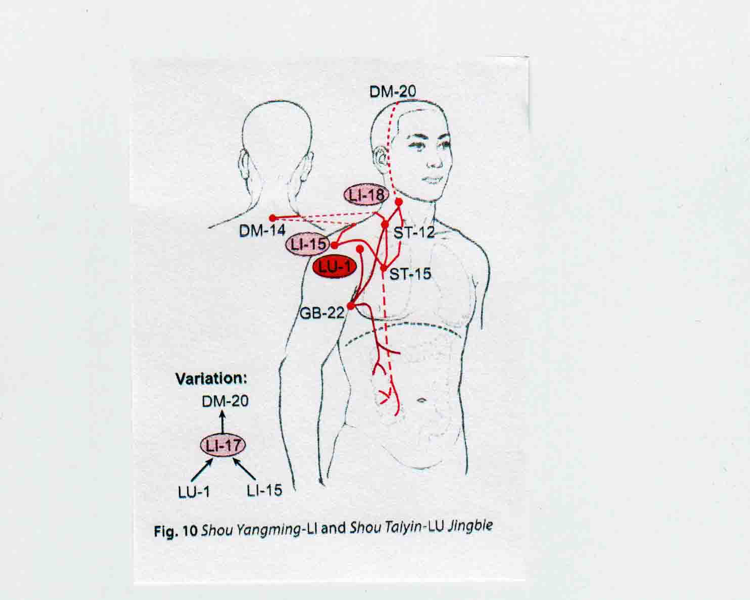 Sixth Confluence LI – LU
BIBLIOGRAPHY
Acupuncture Point and Channel Energetics, Hamid Montakab, Keiner, 2014
The Channel Divergences, Miki Shima and Charles Chace, Blue Poppy, 2001
The Divergent Channels, David Twicken, Singing Dragon, 2014
————————————————————————————————
Sixth Confluence LI – LU
BIBLIOGRAPHY
Acupuncture Point and Channel Energetics, Hamid Montakab, Keiner, 2014
The Channel Divergences, Miki Shima and Charles Chace, Blue Poppy, 2001
The Divergent Channels, David Twicken, Singing Dragon, 2014
————————————————————————————————
 Jake Paul Fratkin, OMD, L.Ac. trained in Korean and Japanese acupuncture since 1975, and Chinese herbal medicine since 1982. He is the author of Essential Chinese Formulas (2014), and Chinese Herbal Patent Medicines, The Clinical Desk Reference (2001). Jake practices in Boulder, Colorado, where he specializes in internal disorders, infections, and pediatrics.
Jake Paul Fratkin, OMD, L.Ac. trained in Korean and Japanese acupuncture since 1975, and Chinese herbal medicine since 1982. He is the author of Essential Chinese Formulas (2014), and Chinese Herbal Patent Medicines, The Clinical Desk Reference (2001). Jake practices in Boulder, Colorado, where he specializes in internal disorders, infections, and pediatrics.
Jake, I always love learning from you. Your recognition and deep understanding of the divergent channel treatment, found within AcuGraph, has been a literal game changer with difficult patients. Thank you for your wisdom!
the best i ever see , excelent job.