Primary Channel Balancing in AcuGraph
In this article, we will be discussing Primary Channel Balancing using AcuGraph. In previous articles prepared for this website, we talked about the Three-Level Acupuncture Balance, which has become my preferred therapeutic protocol for using the AcuGraph system. The three levels are Primary Channels, Eight Extraordinary Channels, and Divergent Channels. The Primary Channels distribute qi and blood, the Eight Extra Channels affect the musculoskeletal body, and the Divergent Channels treat the internal zang-fu organs. This approach is based on Yoshio Manaka and followers, writing in the 1960s, 70s, and 80s, and further developed by Miki Shima in his Somato-Auricular Therapy (SAT) in the 1990s.
I wrote in detail a description of the 3-Level Balance, with separate articles on both the Eight Extraordinary Channel protocol and the Divergent Channel protocol. You can read those articles here, starting with part 1.

The 8-Extra and Divergent balance utilizes ion-pumping cords; the 8-Extra treatment requires four acupoints and will use two sets of ion-pumping cords, and the Divergent treatment also uses four acupoints (a different set), and will use another two sets of ion-pumping cords. Following the ion-pumping-cord treatment of the 8-Extra and Divergent groups, there are often certain meridians that have not been addressed, and are still excess or deficient. This is where we add the Primary Channel balance to complete the treatment.
Click here to purchase ion-pumping cords >>
The 8-Extra and Divergent protocols are combined in the AcuGraph menu as Divergent Treatment. (Use the left, bottom, diverging arrows to access the point recommendations.) Our present article addresses the third wing of this approach, namely Primary Channel balance. It can be used in isolation, as a Primary Channel balance, or added to the 8-Extra/Divergent treatment, completing the 3-Level balance. The 3-Level Balance is preferred in chronic and complicated cases.
The 8-Extra and Divergent balance utilizes ion-pumping cords; the 8-Extra treatment requires four acupoints and will use two sets of ion-pumping cords, and the Divergent treatment also uses four acupoints (a different set), and will use another two sets of ion-pumping cords. Following the ion-pumping-cord treatment of the 8-Extra and Divergent groups, there are often certain meridians that have not been addressed, and are still excess or deficient. This is where we add the Primary Channel balance to complete the treatment.
Cases requiring the 3-Level approach typically have a P.I.E. score below 70, and the lower the P.I.E. score, the more effective and important it is to use the 3-Level approach with ion-pumping cords. When the P.I.E. score is above 70, or even above 65, a quicker and equally effective approach can be accomplished by balancing the Primary channels alone, without paying any attention to 8-Extra or Divergent recommendations. Primary-channel treatment is also important to support dedicated musculoskeletal treatments when the patient is face-down.
In the following paragraphs, we will discuss two different approaches for choosing a Primary-channel protocol. We will first look at the AcuGraph menu recommendations, then will look at Primary channel balancing based on modern protocols from Japan and Taiwan.
AcuGraph Menu Recommendations for Recommendations for Primary-Channel Balance
The AcuGraph menu offers three different primary-channel treatment protocols: the Basic, Advanced, and Expert (under “Treatments”). In each of these treatment protocols, there will be a point recommendation (in blue) below each meridian bar. Sometimes the point is simply the relevant tonification or sedation point. Sometimes, it is a point that will accomplish two tasks at one time. In any case, the point recommendations are based on classical dictates, and you can’t go wrong using any of the recommendations, as long as all of your point choices come from the same grouping, eg, Basic, Advanced, or Expert.
The logic behind meridian balancing is that when the channels are in relative balance – nothing too excess, nothing too deficient – the uninterrupted flow of qi will allow the body to heal itself. Any of the menu recommendations will work, but some menus will be more efficient than others, requiring less needles. I personally think that the preferred goal is fewer needles for maximum balance.
The AcuGraph View Menu
Let’s talk about each of the menu recommendations in isolation, because when you choose points for your treatment, you will probably only need to use one of them. We do this by looking at the graph types offered in the left side menus: Baseline, Yin/Yang, By Element, or Energy Cycle.
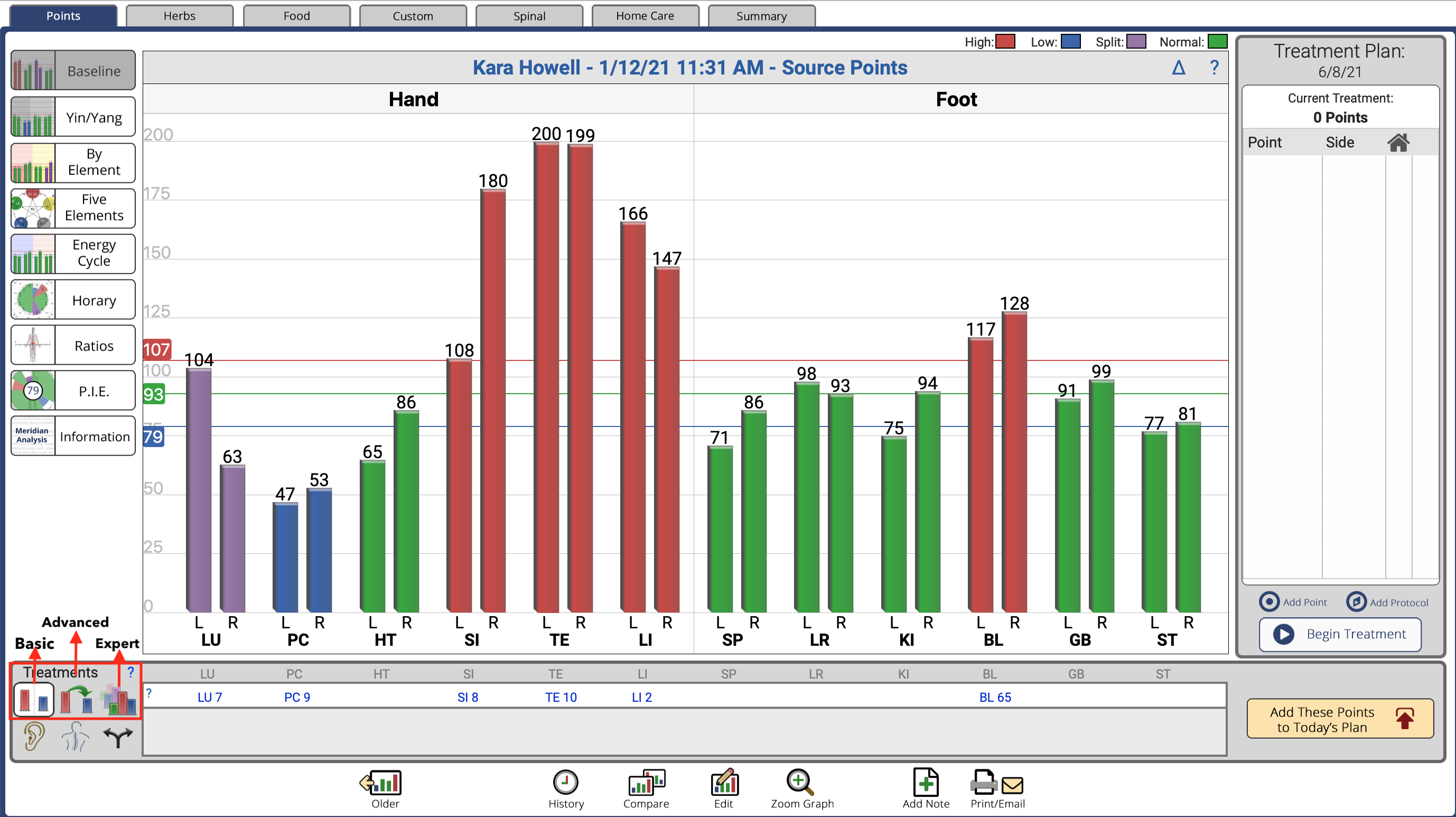
Baseline divides the meridians by hand/upper (on the left) and foot/lower (on the right). This is convenient if you choose points based on working on the arms first or the legs first. In my treatments, I do a shoneishin treatment first (scraping the channels with metal tools), and I will use the “Baseline” graph to allow me to look just at the arms for excess and deficient channels, and then the legs.
Yin/Yang shows the yin channels on the left, and the yang channels on the right. This graph style becomes important if you wish to default to the Keiraku Chiryo treatment, which helps prioritize meridian patterns (more on this later.) For myself, this is the menu I use most frequently.
By Element sequences the channels by their yin-yang partnerships. This becomes important when you want to make sure yin and yang pairs are balanced, leading to either luo-yuan (connecting point-source point) or Divergent treatment. The “By Element” graph, like the “Baseline” graph, is also organized by separating the upper part of the body (left side of screen) from the lower part (right side of screen.)
Energy Cycle shows the meridians in their natural sequence, or in the order of channels in which energy runs through the body. My teacher, Ineon Moon, was always interested in where in this sequence a blockage occurred. This would be seen as one or more excess channels (red bars) preceding a significant drop to one or more deficient channels (blue bars). His solution would be to use the luo-connecting point of the last excess (red) channel before the drop to deficient (blue), allowing the normal flow to continue. If the two channels were part of a pair (eg Stomach excess and Spleen deficient), he would use the luo point of the excess channel and the yuan-source point of the deficient channel. The Manaka approach used ion-pumping cords to lead the excess into the deficiency.
Treatments
Once you have chosen your graph view, you now can go to “Treatments” for appropriate point recommendations. In the bottom left of the screen, we have six icons for “Treatment”. The top three icons will contribute to Primary Channel balancing.
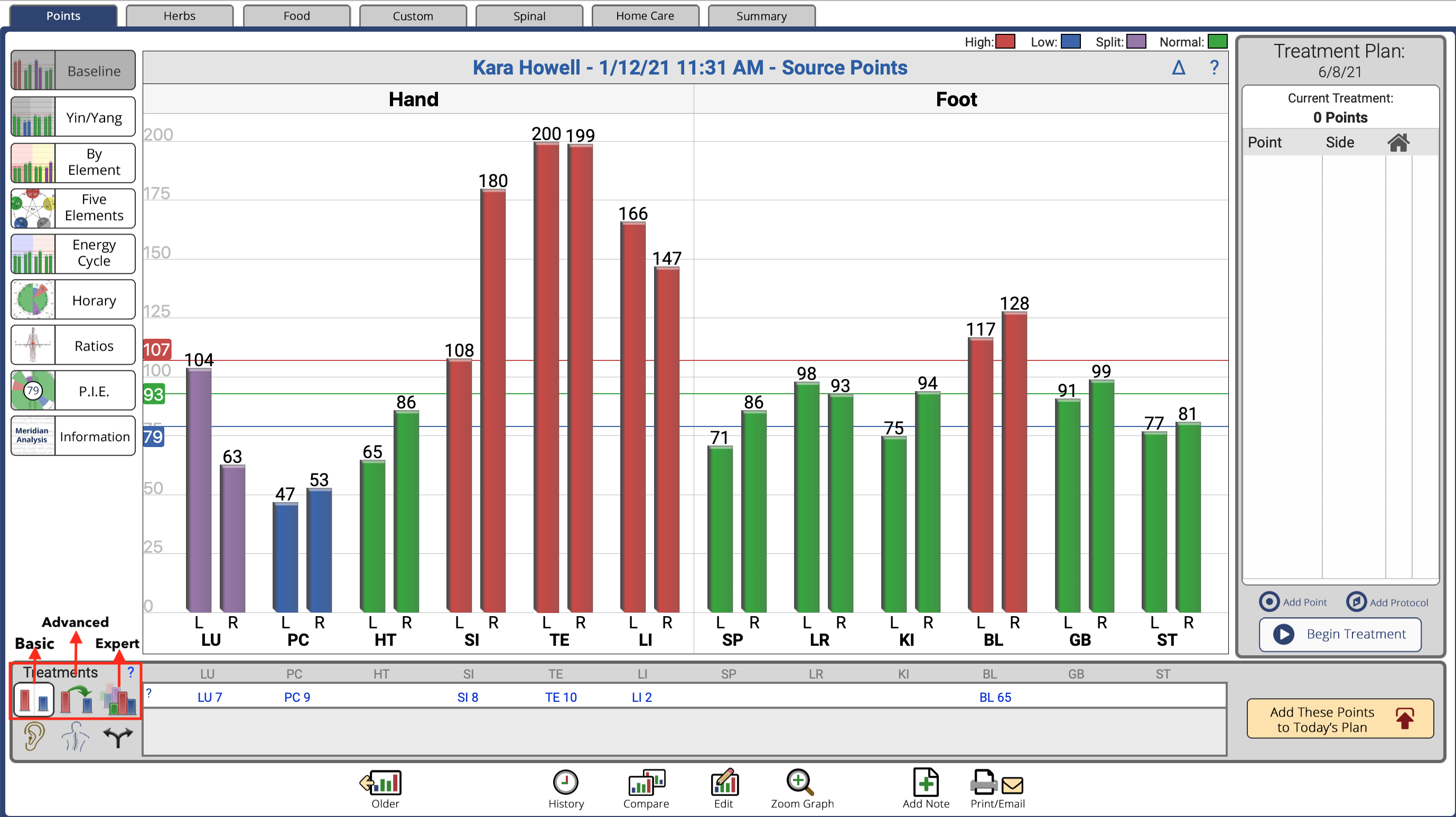
The bottom right, the diverging black arrows, will lead you to the 3-Level Balance points for balancing 8 Extra and Divergents. (I have discussed this approach in previous articles.) Here, we will concentrate on the top 3 treatment icons, in order to balance Primary Channels only. As a reminder, I tend to use this approach when the P.I.E. score is greater than 70, though I prefer the 3-Level Balance with ion-pumping cords for more complicated cases and lower pie scores.
I also choose one of these primary-channel point recommendations when I am treating the back for musculoskeletal problems, regardless of the P.I.E. score. These menus allow me to add tonification or sedation points of the most affected channels, allowing a balance treatment to be combined with a musculoskeletal treatment. The tonification and sedation points are always below the elbow or knee, and can easily be added to a back-torso treatment. Plus, this avoids any awkwardness of managing the ion-pumping cords with the patient prone. I will also use the Primary balance as a stand-alone treatment (without 8-Extra/Divergent) in any case where I don’t want to use ion-pumping cords, or to do quick excess and deficient treatments with laser.
Options in AcuGraph
Basic. This approach tonifies deficient meridians, sedates excessive meridians, and addresses L/R imbalances using Luo points. It is an effective treatment, but not very efficient, using more needles than may be necessary.
Advanced. This approach enhances the Basic treatment by adding Shen, Ko, and Luo transfers to accomplish more, using fewer points. It also includes group treatment points and global pattern treatments. Here, we will get point recommendations that might apply one point to several channels. In this regard, it is a more efficient balance. I usually default to this menu.
Expert. This approach enhances the Advanced treatment by considering the patient’s prior graph patterns and imbalances, in selecting treatment points. It also considers exams of different types (Source, Jing-well) performed on the same day. Some practitioners like including the patient’s historical patterns for input in the treatment plan.
Personally, I tend to work in either Advanced, or Divergent.
For any of the three choices, point recommendations are provided in a white horizontal bar, below the channel bars. In all the treatment approaches, we have the ability to ask “Why? Why this point?” The answer is found by clicking on the question mark (?) to the very left of the point recommendations. Some points will apply to two or more channels, and the reason is provided. For example, SP 4 might be used for both Spleen deficiency, and Stomach excess. Or it lists a Luo point, or an element point, etc.
Once you have chosen your Treatment, you can enter the points into the Treatment Plan by clicking “Add These Points to Today’s Plan,” at the lower right. The AcuGraph menu allows you to remove (the X in the red circle) or add your own points (“Add Point”). This feature is convenient for creating a computer-stored record of your treatment.
So here we have, in the AcuGraph menus, three ways to balance the channels, with point recommendations. All of the recommendations are based on classical applications of tonification, sedation, luo-connecting, yuan-source, five phase (elements), etc. And each method works.
Why AcuGraph Matters
One of the beauties of the AcuGraph program is visually showing relative excesses and deficiencies. This gives us flexibility beyond the AcuGraph treatment recommendations. For example, we may just want to know the most excess channels, or the most deficient, and work with those. This is what I recommend when doing a musculoskeletal treatment. Also, when I do the 3-Level Balance (which concentrates on 8-Extra and Divergent treatments), I want to know which channels have not been included, and not been treated. This is where I bring a Primary Channel balance into play, allowing me to complete my treatment.
Now that we’ve had a refresher on the Primary Channel balancing methods, we’ll delve further into more advanced applications of this method in the following sections.
Thanks for Reading.
Modern Japanese and Chinese Approaches to Balancing Acupuncture Meridians
Relationships of acupuncture meridians (channels) have been mapped out since the Nan Jing (100 CE). The essential premise is that qi (life energy) flows through twelve channels in a continuous sequence. This energy nourishes and invigorates all tissues along each pathway, including designated organs (zang-fu), blood flow, muscle, bone, etc. Health problems occur when that flow is either interrupted (blocked), or when the quality of the qi and blood is sub-standard. In the Nan Jing, pathway acupoints were described that allowed an intervention/manipulation of the channel, using needle or moxa. Channels could be controlled directly by reducing, supplementing, heating, or cooling. Or, points could be chosen that allowed connection to one or more other channels.
The Nan Jing establishes the importance of the acupuncture meridians network, describing its pathways as well as the locations and functions of the acupoints. It also described the basis of meridian balancing, that all channels need to have relatively equal amounts of qi, and that this balance can be achieved by using certain groups of acupuncture points to connect the channels directly.
The goal of the acupuncturist is to determine which channels have too much energy (excess), and which channels have too little energy (deficient), and then choose certain acupoints to rectify the channel flow. All the various schools of meridian balance follow this dictate, whether they originate in China, Taiwan, Japan, Vietnam, Korea, Europe or North America. This can be done by leading excess to deficiency with ion-pumping cords (in Manaka style), by adjusting each channel individually according to excess /deficiency with relevant acupoints, or by using specific points that can interface between two (or more) channels.
Proper Diagnosis
Obviously, the first requirement for meridian balance is proper diagnosis of which channels are out of balance, as either excess or deficiency. Traditionally, this was done by evaluation of the radial pulse on the wrist (or other locations), and later, in Japan, by skin or abdominal palpation. Our earlier Asian doctors were extremely sensitive and advanced in their pulse diagnostic abilities. I have seldom seen modern Western practitioners obtain the level required to make accurate diagnosis of specific meridian imbalances. Chinese herbalists, on the other hand, concentrate on whole pulse diagnosis, and are able to distinguish 28 aberrant pulses.
This is suitable for herbal prescribing, and many Westerners have mastered this level. But to distinguish excesses and deficiencies of all twelve of the meridians on the radial pulse is difficult. I used to teach meridian pulse diagnosis, and I feel I was as good as many at this. But after nine years of using AcuGraph, I am convinced that computer diagnosis is much more accurate, and more revealing of the subtleties of comparative meridian strength.
In any event, the idea of evaluating and treating meridian imbalances was in place at the time of the Nan Jing, and persisted through many centuries in Eastern Asia. By the time of the founding of the People’s Republic of China, however, the art of balancing acupuncture meridians disappeared. When China organized its TCM universities and medical schools in the 1950s, it put into place the acupuncture protocol based in zang-fu and Eight Category diagnosis and treatment. This dove-tailed with the curriculum organized by the TCM herbalists, allowing a unified teaching program. Any school of thought focusing on meridian therapy was therefore lost in mainland China, but certain schools survived outside in Japan, Taiwan, Hong Kong, Korea, Vietnam, and later, Europe and North America.
Keiraku Chiryo, Japanese Meridian Balancing
The revival and flowering of Nan Jing meridian balancing occurred in Japan in the 1930s, in a conscious effort by a group of dedicated acupuncturists. They called their system Keiraku Chiryo (School of Meridian Therapy). (For a more complete overview and history, see www.drjakefratkin.com/keiraku-chiryo/). I followed this approach for 25 years, and studied with several of its leading modern-day proponents from Japan. There is a take-away from this approach that I now incorporate into the 3-Level Balance with AcuGraph. Whether we focus on the Divergent treatment (P.I.E. score below 70), or Primary Channel balance only (P.I.E. score above 70), I always look for the Keiraku Chiryo organization to determine the Primary Pattern (sho), the pattern underlying all the other imbalances.
In Keiraku Chiryo (KC), the Primary Pattern is determined by pulse diagnosis. It starts by determining which acupuncture meridians are deficient, and which are excess. On the AcuGraph screen, of course, we can visually see this for every channel. (We should just consider the blue and red bars, by the way, and not the split-purple bars, or greens.) KC determines a primary pattern, which basically is the origin behind all of the other channel imbalances. (The Worsley Five Element method is based on the KC system, and they call the Primary Pattern the Causative Factor.) KC feels that if we can identify this prime imbalance, we can fix all of the channel imbalances.
In classical Keiraku Chiryo, four patterns are possible, all restricted to the yin channels: Spleen, Lung, Kidney and Liver. (Heart and Pericardium were excluded.) Unlike the Worsley system, which considers Primary patterns (Causative Factor) to underlie a patient’s constitution throughout much of their lives, and subsequently, through most of their treatments, the reading on an AcuGraph patient reveals that the primary imbalance probably changes every two hours. Our AcuGraph reading is a snapshot of a moment in time, telling us what is out of balance now. If we address the present imbalance, even if it is only a two-hour window, this will allow a reset to occur during the following 24-hour period. When we restore the flow of qi, unobstructed, the body heals itself.
We cannot say that today’s pattern in the acupuncture meridians reveals a deep constitutional statement, unless the pattern constantly repeats itself. We only know this by comparing our reading to previous readings. (Use the “Compare” icon on the bottom white bar.) Patients often ask to do another reading immediately following the treatment to see if there is improvement. I tell them it takes 24 hours for the repair to show itself, for the meridians to go through their 24-hour cycle.
Don’t Forget The Primary Pattern
In practice, I feel it is always important to make sure that a treatment for the KC Primary imbalance is included. If we are doing the 3-Level Balance (the Divergent treatment), it may be that the Primary Pattern is already included in our point recommendations, in which case we don’t have to add anything. If it is not included, we should add points to address it. If we are only focusing on a Primary Channel treatment, and not doing the complete 3-Level balance, then we definitely want to make sure that the Primary pattern is addressed.
How do we determine the Primary pattern? In a nutshell, we are looking for a specific pattern of deficient channels (blue) that belong to the yin channels, namely, HT, PC, SP, LU, KI, and LR. [For the moment, we ignore the yang channels (SI, TE, ST, LI, BL, GB)]. We are not looking for the most deficient yin blue bar, but rather, where the blue bars are in relationship to each other.
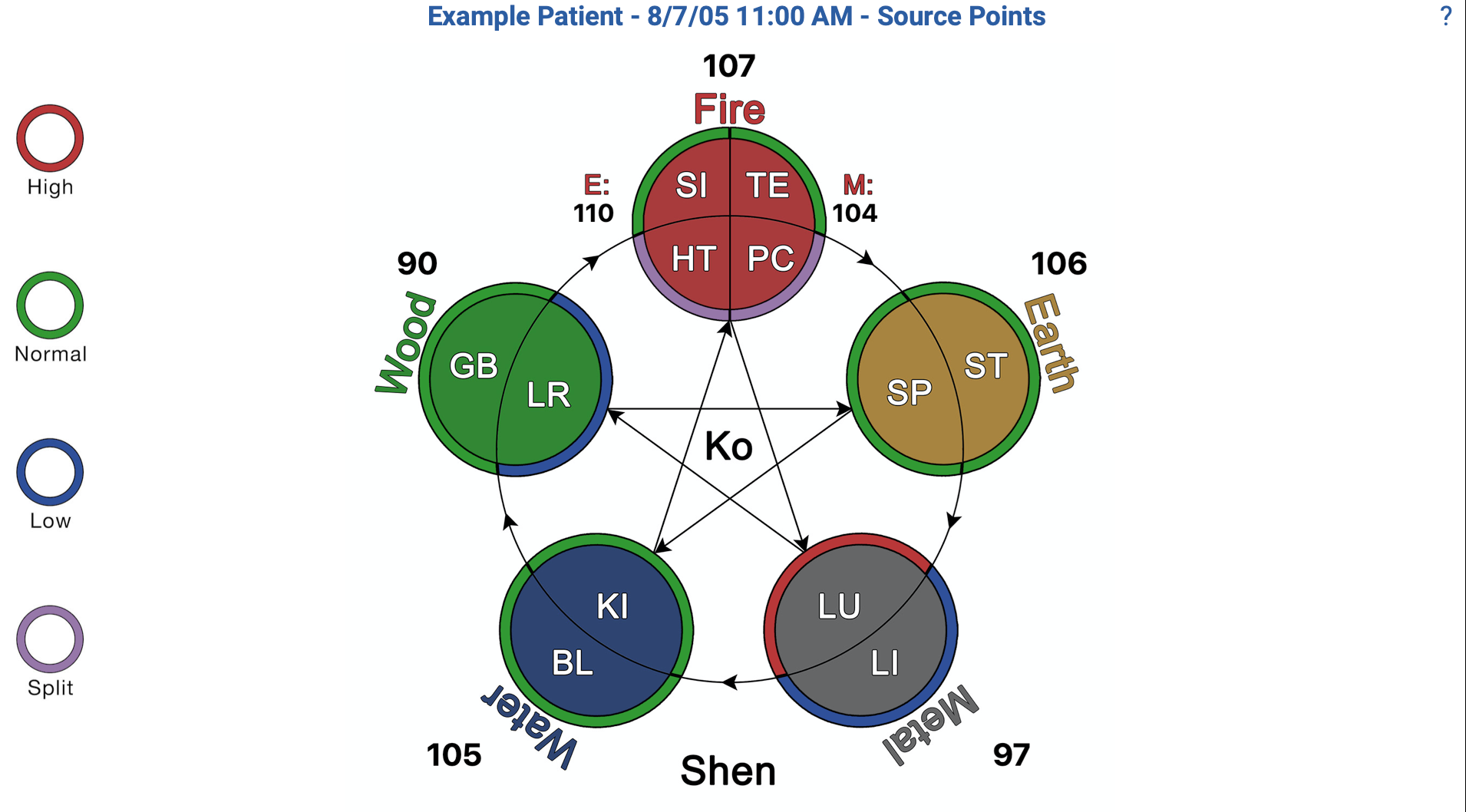
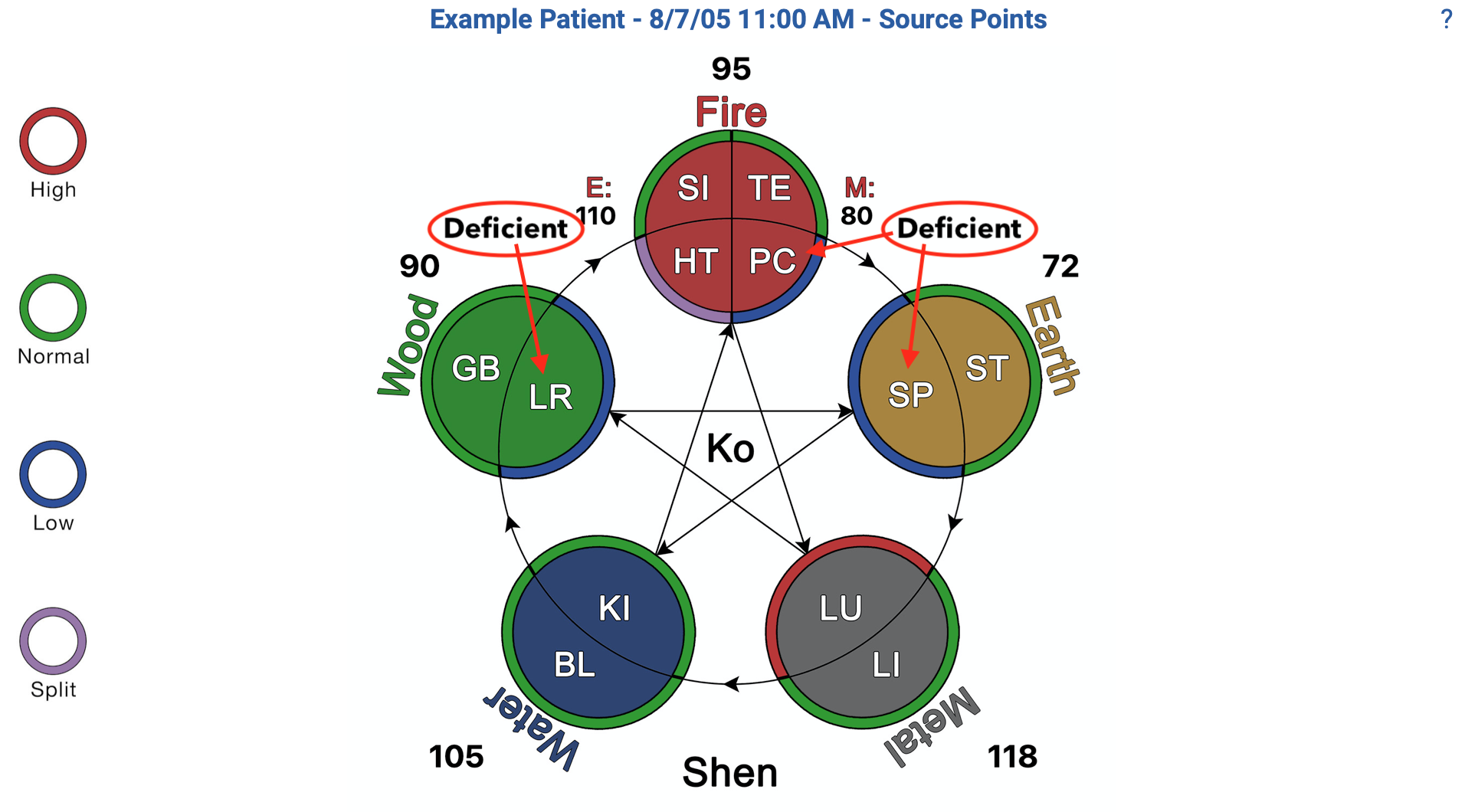
This is easiest to visualize on the 5-elements chart pictured above. In this chart, there is a clockwise sequencing of elements, with yin channels on the inside of the circle and yang channels on the outside. Each channel is colored accorting to its element (fire=red, wood=green, etc.) and each channel is outlined with the color representing its status. For example, a deficient LR channel will be shown in green (wood) with a blue outline (deficient.)
In this presentation, we are looking for the most distally-clockwise deficient yin channel, most often preceded by another blue deficient yin channel. That is to say that typically, there will be two blue outlines in sequence. For example, a graph may show LR and KI being blue (deficient) and SP being blue or red. LR and KI are next to each other in the 5 Element sequence, with KI being the mother of LR. In this case, LR is the primary pattern. The last deficient channel (blue) on the clockwise cycle is the primary! This is easiest when two blues are together. Choose the last one most clockwise. If three blue bars are together, still, choose the most clockwise bar as the Primary Pattern. If no two blues are together, you can treat all of the blue bars, or concentrate on the most deficient.
Another example, illustrated below. The 5-elements chart shows blue outlines for PC, SP, LR. (Remember: Ignore the reds, purples and yang channels.) In this example, PC and SP are in sequence, PC being the mother of SP. LR is off on its own. Spleen is therefore the furthest clockwise deficient channel.
Once we identify the Primary channel, our goal is to tonify it, and we can do that in numerous ways. The easiest is to use the tonification point of that channel, but we can also use the yuan-source point, or the horary point (the element point of the channel), e.g., the fire point of the Pericardium channel, or the water point of the Kidney channel. Strict followers of KC also tonify the mother channel of the affected channel, but I have found (through my own finger muscle-testing) that treating the primary alone is usually enough. When a Primary channel (according to KC) is not addressed in our more complete Divergent treatment, I would also add tonification of the Primary channel to the treatment. If we are doing a Primary Channel balance only, I would start by making sure the KC channel is included.
“Don’t Chase Every Meridian Imbalance”
Kodo Fukishima, one of the early masters of Keiraku Chiryo, advised “Don’t chase every meridian imbalance. If you focus on the primary, this will take care of all channels out of balance.” This tells us to how to do effective balancing of acupuncture meridians without treating every channel that is excess or deficient. Although I don’t simplify as much as Fukishima recommends, I avoid treating every imbalance, and instead concentrate on the most egregious. I will tonify the deficient primary channel according to KC; but I also tonify any other deeply deficient blue yin channel, and sedate the most egregious red excesses. This is contrary to Fukishima’s advice, but it is what I do.
Also, through clinical practice and using my O-ring muscle testing, I have found that if a meridian is excess or deficient on both sides, treating only one side actually treats both sides. In my opinion, it is unnecessary to treat both sides.
Summary
Let me repeat and summarize. If the P.I.E. score is above 70 (or even 65), I will choose to balance the Primary Channels only (without 8-Extra/Divergent). I do this by looking at the 5-element graph to determine the most clockwise yin deficiency (outlined in blue). Most primary patterns will show two adjacent yin channels being deficient (blue), and I chose the furthest clockwise channel. If SP, PC and LR show blue, the primary pattern is SP (not LR!) This is because PC comes right before SP on the 5-element diagram, and LR comes before PC.
So, having identified the Primary yin deficiency, I tonify that channel, usually with the tonification point. (I can also use the yuan-source point or the horary point.) However, in most cases, there are significant blues and reds on their chart. I will often identify other blues and scattered excess reds. I will choose the worst of the blues and reds, and try to balance with ion-pumping cords, if possible.
The Taiji Balancing Method
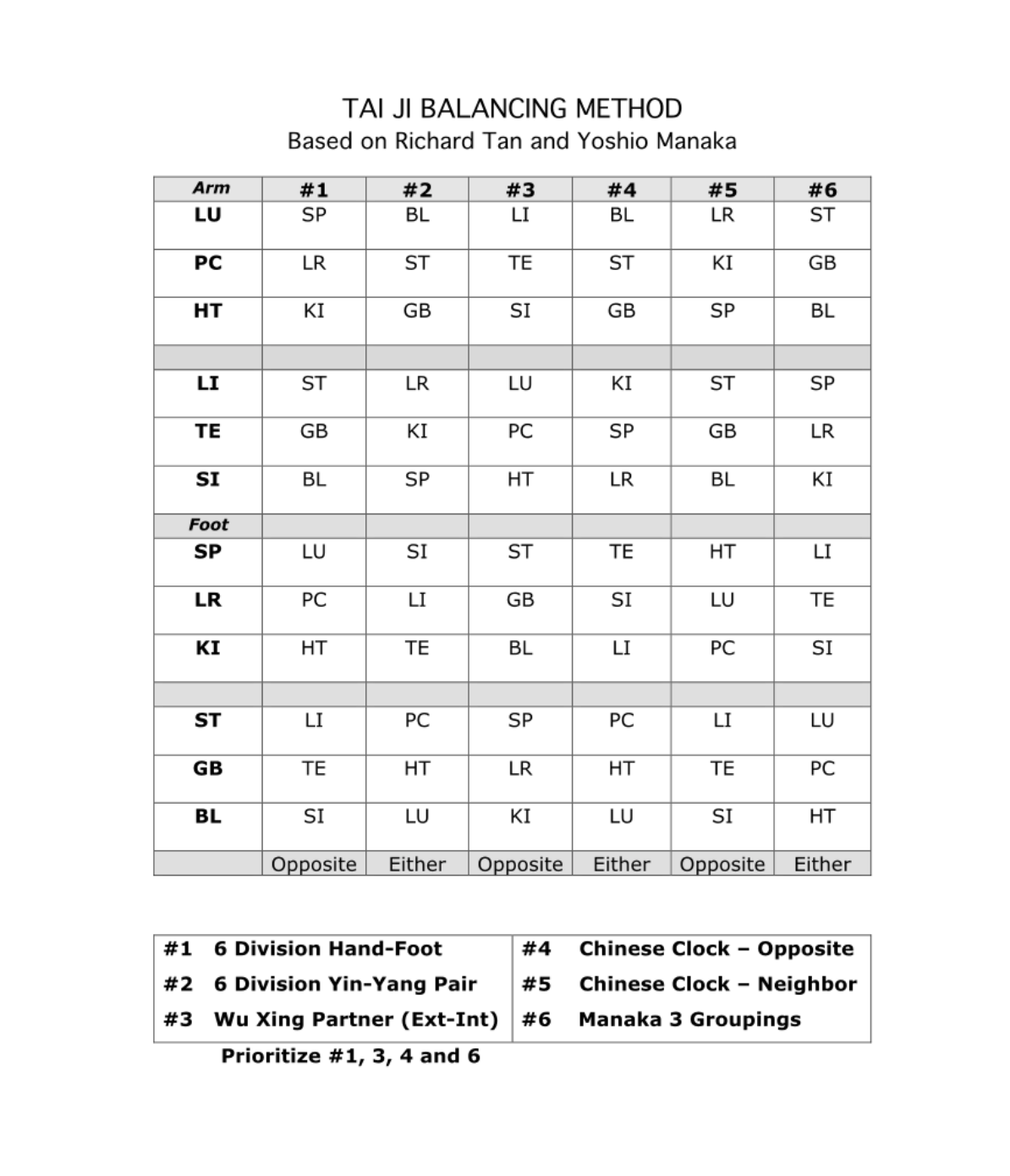
When there are lots of channels out of balance, we really don’t want to be chasing every one (following Fukishima’s dictate.) So, what should we do? I have a clever solution: I use ion-pumping cords to connect the more extreme deficiencies with the more extreme excesses. In this case, we have guidance in the form of a chart called the Taiji Balancing Method (see below.) This chart lists classical relationships that can be used for this purpose. First organized by Dr. Richard Tan, from Taiwan and later California, the chart delineates five classical relationships. To this, we added a sixth, proposed by Yoshio Manaka.
To read the chart, the left column lists the channel you wish to balance, with six channels in columns to the right, based on different classical relationships. These relationships are used to balance a deficient channel with an excess channel. Your channel in the most left column can be either excess or deficient, as long as the channel chosen from the right-side columns is the opposite, eg, excess vs. deficient. We use ion-pumping cords to lead the excess channel (black lead) towards the deficient channel (red lead). You will have to decide which actual point to use, but common pairings are tonification to sedation or luo-connecting to yuan-source.
The Six Relationships
#1: Six Division Hand-Foot
These channels are placed geographically: medial, middle, lateral. Here, a hand channel is paired with a leg channel by the six-division organization: Taiyin (LU-SP), Jueyin (PC-LR), Shaoyin (HT-KI), Yangming (LI-ST), Shaoyang (TE-GB) and Taiyang (SI-BL). This relationship is commonly chosen.
#2: Six Division Yin-Yang Pair
This is a more obscure relationship, based on the couplings of the six divisions according to yin and yang. The sequence can be visualized on the Yin/Yang menu, left side of the AcuGraph page. LU-BL (Taiyin-Taiyang), SI-SP (Taiyang-Taiyin), HT-GB (Shaoyin-Shaoyang), TE-KI (Shaoyang-Shaoyin), PC-ST (Jueyin-Yangming), LI-LR (Yangming-Jueyin). Incidentally, this is the meridian coupling preferred in Master T’ung’s acupuncture system, as detailed by Dr. Wei-Chieh Young in “Lectures in Tung’s Acupuncture”. They applied contralateral needling.
#3: Wu Xing (Five Element) Partner; External-Internal
This couples the yin and yang partners of each element. LU-LI (Metal), PC-TE (Ministerial Fire), HT-SI (Fire), SP-ST (Earth), LR-GB (Wood), KI-BL (Water). These pairings can be visualized using the Five Element menu on the AcuGraph page.
#4: Chinese Clock – Opposite
For reference, use the Horary menu of the AcuGraph page. This balances two channels by crossing over to the relevant channel on the other side of the day. LU-BL, PC-ST, HT-GB, LI-KI, TE-SP, SI-LR. These can be directed in either direction. My teacher Dr. Ineon Moon liked using this combination, if he knew that both partners were in obvious excess-deficiency.
#5: Chinese Clock – Neighbor
These channels are adjacent to each other in the bioclock sequence, and work well in blockages. LU-LR, KI-PC, SP-HT, LI-ST, TE-GB, SI-BL.
#6: Manaka 3 Groupings
Yoshio Manaka saw three fundamental pairings of yin and yang channels, which he felt represented continuous circuits of paired meridians. Each group has four channels, two pairs. Two of the points connect as the Wu Xing/Five Element pair (#3). The other pair is determined by a cross-over link, represented in this graph and listed as #6:
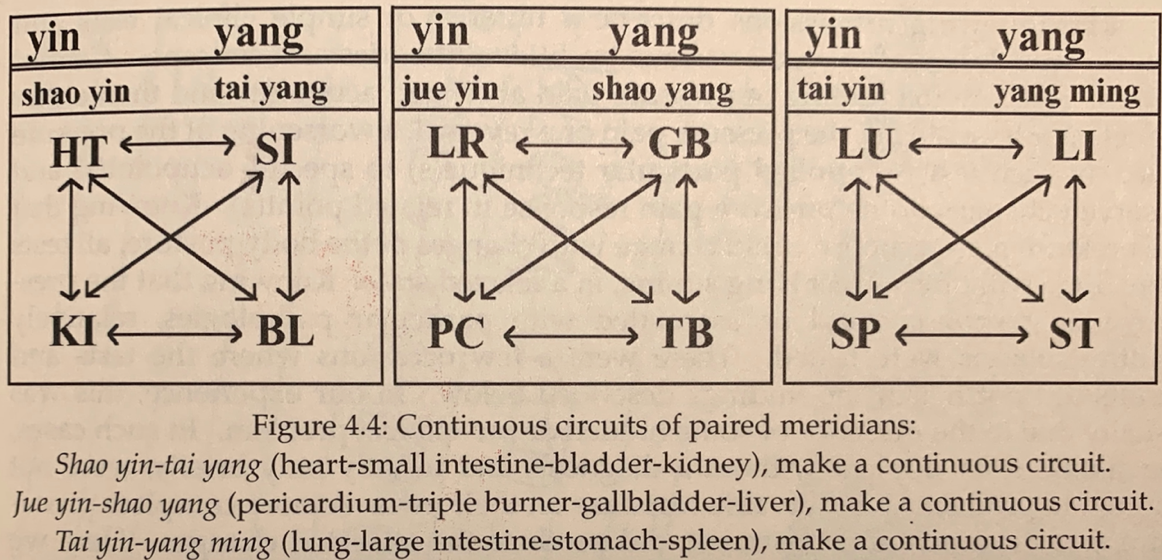
The image about is from Chasing the Dragon’s Tail, Yoshio Manaka, Paradigm Publications, 1995, 2014, p. 59
Summary
In summary, the idea is to use one of the six groupings on the Taiji Balancing Method chart (above) to pair a more extreme channel excess with a more extreme channel deficiency, using ion-pumping cords. In practice, #1, 3 and 6 are used most often, although I like and use any of the pairings. I think they all work! The pairings should connect an obvious excess channel with an obvious deficient channel (black lead on the excess, red lead on the deficient). But the partner chosen should be included on the Taiji Balancing Method chart. By using ion-pumping cords, the balance is made most efficiently.
This means looking at all the possibilities. For example, if KI is weak/deficient, look at the chart to see if any of the six possibilities are particularly excess, and use that one. You don’t want to connect to a green (normal), and you don’t want to connect an excess to an excess, or a deficient to a deficient.
The following section provides actual treatment examples to apply these concepts.
Treatment Examples
In the first three parts of this series, we looked at several meridian channel balance approaches. In today’s post, we’ll apply what we’ve learned with some actual treatment examples.
Treatment Example 1.

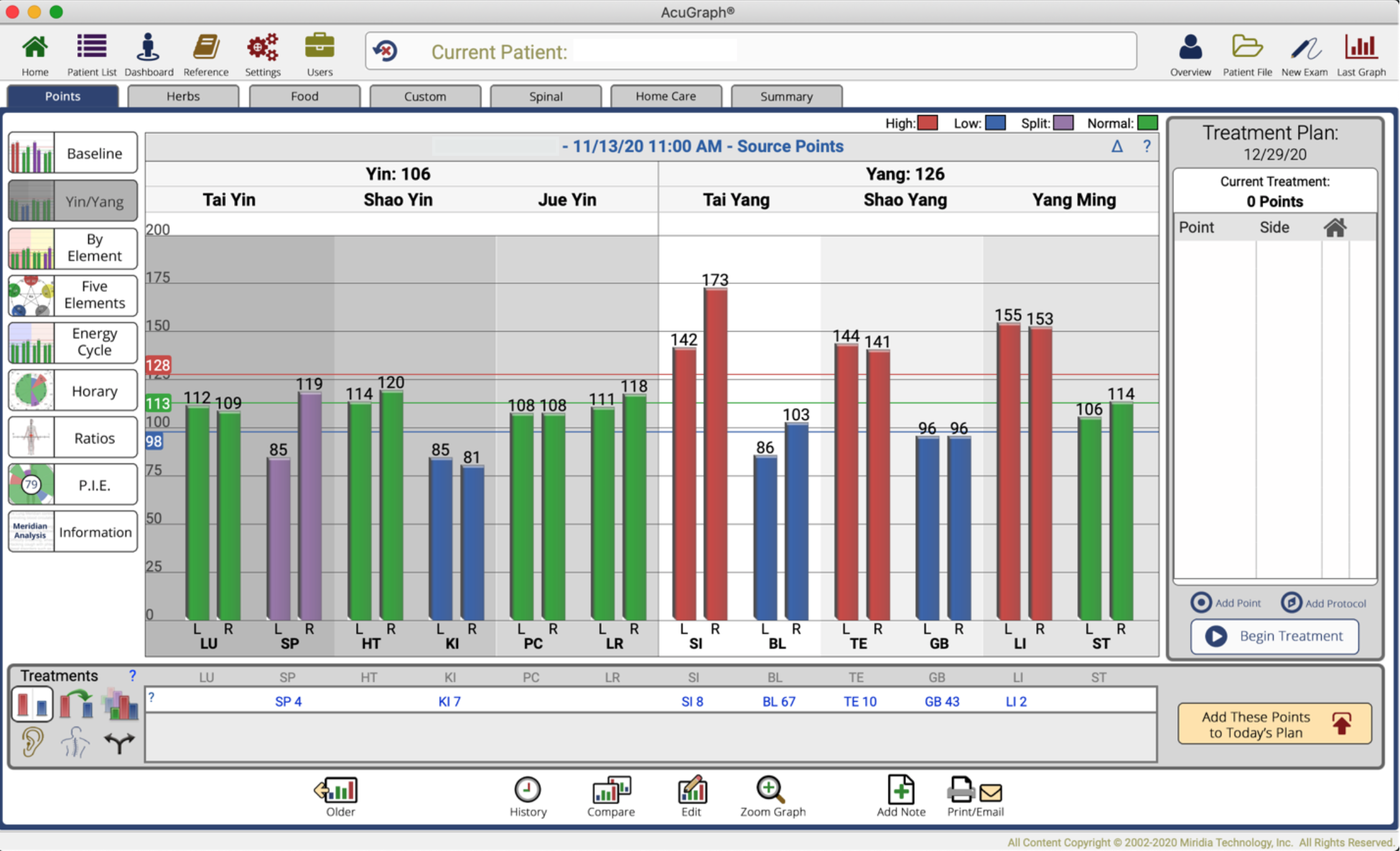
The above screen is in the Yin/Yang graph, allowing us to determine the Primary Pattern of the six yin channels, on left side. We see that SP, PC, and LR are all blue, meaning deficient. Which blue represents the primary? Imagine the 5-Element sequence, going clockwise.
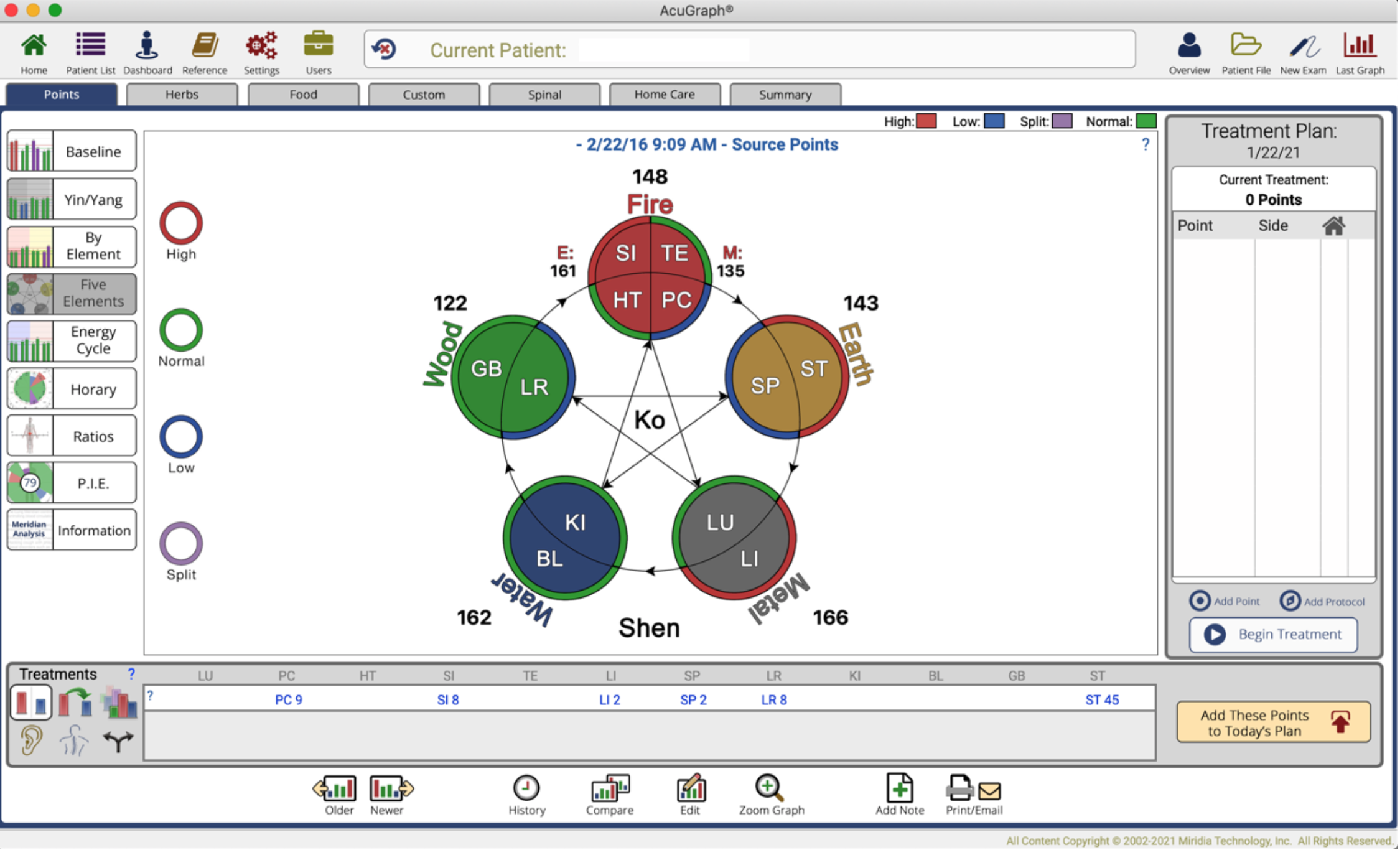
The order would be LR, PC, SP. (In this chart, PC is called Circulation/Sex). We look for any two that will be adjacent to each other (mother and child). LR and PC are adjacent, but so is PC and SP. SP is the most clockwise blue on the yin channels, and its mother (PC) is also blue, so SP is the primary. Had SP not shown, but instead LU did, then PC would be the primary. (Classical Keiraku Chiryo does not recognize HT or PC as primary patterns, but I do, based on clinical practice.) Now that we know SP is the primary pattern, we want to make sure it is tonified in our treatment.

If I choose to simplify and use ion-pumping cords, I would make sure to treat the KC primary, which is SP. Looking at our Taiji Balancing Method Chart (below), I would go to the SP column on the left, and then see if any of the point recommendations in the 6 columns to the right are particularly excess. To this end we see that 3 of our groups offer a red excess: SI (#2), ST (#3), and LI (#6). Which one to choose? For one thing, degree of excess is important, and in that regard right sides of both ST and LI are the higher. Additionally, LI fulfills Manaka’s priority. So, either one would work, and would be the channel that is sedated (black clip) while SP receives the tonification end of the ion-pumping cord (red clip).
In addition, I would tonify LR on the left side, because it is significantly low. I would ignore PC and SI because they are only slightly out of normal range. And in this case, I look at my Taiji Balancing Method chart, trying to find what could balance out left side LR. Either the excess on SI (#4) or the excess on LI (#2) will work. To balance, I can mix left and right sides, if necessary, with my ion-pumping cord. But in this case the red excess of LI and SI are not particularly excessive. It would just as well work to go with tonifying LR on the left side with the AcuGraph menu recommendation, LR 8, and not bother with another cord.
Case #2.
Here is a simple case. The P.I.E. score was 60. If we look at the Yin/Yang graph, we have one meridian, KI, in blue. SP is also showing deficient on the left side. So, we can say that KI is the primary. It can be treated in isolation with its tonification point, or we use ion-pumping cords to feed in one of the excess yang channels. There, our choices in red are SI, TE, and LI. Looking then at the Taiji Balancing Method chart, to KI in the furthermost left column, we find as available partners: SI (#6), TE (#2), and LI (#4). We could use any of these to tonify KI. My preference would be for Manaka’s 3-Group recommendation, SI, and a second choice would be Chinese clock opposite, LI.
Having included that, I also would tonify SP on the left side. We can do this in isolation, with a SP tonification point, or we could attach by ion-pumping cord to SI (#2), TE (#4), or LI (#6). Since we have chosen SI to balance KI, then we can choose TE or LI. The tonification would happen on the left side, which is the deficient side on the SP channel.
In general, I like to cross the body when moving an excess into a deficiency.
In conclusion, proper Meridian Balancing should prioritize which deficient and which excess channels to treat. Concentrate on the primary according to Keiraku Chiryo, but also seek to return to normal the most extreme excess(s) and the most extreme deficient(s). When the qi is of good quality, and can run unobstructed through the channels in their natural sequence, health and well-being are restored.
I hope this article was helpful. Thanks for reading!
3 Replies to “The Primary Channel Balance”